569126
Question 1
Question
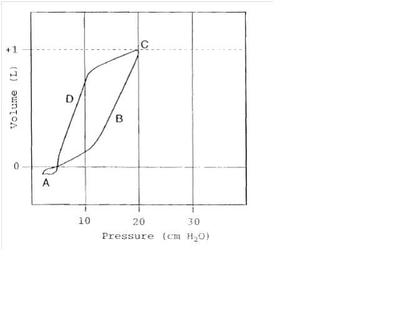
The inspiratory flow limb of this pressure volume curve is indicated by which letter?
Image:
question_1.JPG (image/JPG)
{kind=link}
Answer
-
a
-
b
-
c
-
d
Question 2
Question
Which of the below steps should improve ventilation and clearance of CO2?
Answer
-
Lowering the tidal volume from 10 cc/kg to 8 cc/kg PBW in Volume Assist Control
-
Decreasing the flow rate from 80 L/min to 50 L/min in Volume Assist Control
-
Increasing the Inspiratory time from 1 sec to 3 seconds in Pressure Assist Control ventilation
-
Increasing the respiratory rate from 12 to 15
-
Increase PEEP from 5 to 10
Question 3
Question
Your patient has a baseline plateau pressure of 20, peak pressure of 23. Suddenly, his peak pressure alarms goes off. Now, his plateau pressure is 22 and his peak pressure is 33. Which of the following list of possibilities would cause these changes in peak and plateau pressures?
Answer
-
Acute Bronchospasm
-
Pneumothorax
-
Flash pulmonary edema
-
Right Mainstem Intubation
-
Large mucus plug causing complete Left lower lobe collapse.
Question 4
Question
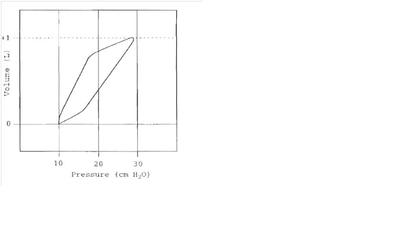
Based on the curve above, what minimum level of PEEP would be necessary to prevent alveolar collapse at end-expiration?
Image:
PEEP_needs.JPG (image/JPG)
{kind=link}
Answer
-
10
-
12
-
16
-
20
-
28
Question 5
Question
How do you assess for increasing resistance in the ventilator circuit?
Answer
-
The flow volume curve shows bird beaking
-
The pressure volume curve changes angle
-
Your difference between Plateau pressure and PEEP increases
-
The difference between Peak pressure and Plateau pressure increases
-
The difference between Peak pressure and PEEP increases
Question 6
Question
Your patient is recovering from severe ARDS with improving lung compliance and oxygenation over 4 days. Which of the below scenarios is expected if NO changes are made to the patient’s current ventilator settings?
Answer
-
In Volume Assist Control, increased patient respiratory rate compared to set frequency on ventilator
-
In Volume Assist Control , peak pressure decreasing from 40 to 30 but plateau pressure staying the same at 28
-
In Pressure Assist Control ventilation, increasing tidal volumes over time
-
Worsening hypercapnia and lowering of the pH
-
In Synchronized Intermittent Mandatory Ventilation, the number of control breaths decreases as the patient begins to trigger more frequent breaths
Question 7
Question
A 34 y/o male patient with past medical Hx of asthma is brought to your ICU from an outside hospital intubated and on mechanical ventilation. His current settings are: Volume Assist Control - f: 10, PEEP: 5, Vt: 500 and FiO2: 60%. The patient’s vitals are: temp: 37.8, HR: 118, BP: 89/40, RR: 26, sat: 93%. His ABG shows: pH: 7.31/ 48/89/22/Sat: 91%. At the bedside, you note a young man who is sedated, has increased WOB, + decreased airflow with high pitched inspiratory and expiratory wheeze.
Which of the below interventions would most likely improve your patients clinical status?
Answer
-
Decrease the inspiratory flow rate from 90 L/min to 60 L/min
-
Check the ventilator for autopeep and increase the PEEP to 5 points higher than the calculated autoPEEP to reduce the effort for initiating respiratory triggering
-
Change the patient to Pressure Assist Control Ventilation and extend the Itime for each breath
-
Increase the PEEP to 15 to improve oxygenation
-
Disconnect the patient from the ventilator for a few seconds to allow complete expiration
Question 8
Question
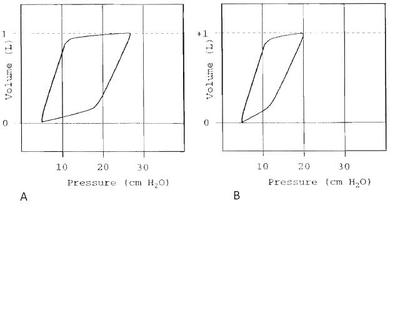
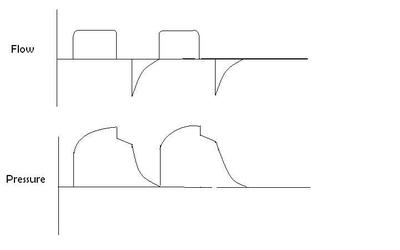
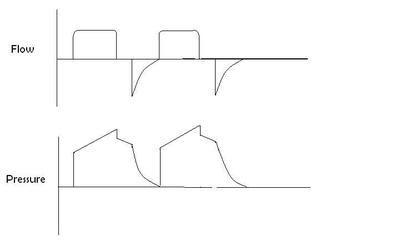
Please choose the best answer that describes the relationship between both curves.
{kind=link}
Answer
-
You can’t define any differences in compliance or resistance from P/V curves
-
Curve A has increased compliance compared to curve B.
-
Curve B has increased compliance compared to curve A.
-
Curve A has increased resistance compared to curve B.
-
Curve A has a decreased resistance compared to curve B.
Question 9
Question
Your patient has a baseline plateau pressure of 20, peak pressure of 23. Suddenly, the vent is alarming for high peak pressures. Now, his plateau pressure is 29 and his peak pressure is 33. Which of the following list of possibilities would cause this change in peak and plateau pressures?
Answer
-
The patient biting down on the ETT
-
Squamous cell cancer at the level of the carina with endophytic mass causing acute large airway (R mainstem) obstruction with associated right lung atelectasis
-
The ventilator tubing getting squished in the edge of the bed during movement, causing obstruction of flow
-
Gradual worsening of ARDS with slowly worsening atelectasis on CXRs over 3 days
-
Bronchitis patient requiring frequent suctioning due to copious secretions
Question 10
Question
You have decided to use the stress index as a measure of the appropriate PEEP needed to prevent alveolar collapse while minimizing alveolar overdistension. What criteria below must all be met?
Answer
-
Patient presents with a COPD exacerbation. He is on mechanical ventilation using Volume Assist Control, a decelerating ramp waveform, and the patient is sedating and not triggering his own breaths.
-
The patient presents with diffuse ARDS due to sepsis, he is being ventilated on Volume Assist Control ventilation with a square waveform, he is awake and triggering his own breaths.
-
The patient has focal ARDS with primary pneumonia, he is not triggering his own breaths, and he is on Volume Assist Control ventilation with a decelerating ramp waveform.
-
The patient has focal ARDS with primary pneumonia, he is not triggering his own breaths, and he is on Volume Assist Control ventilation with a square waveform
-
The patient has diffuse ARDS due to sepsis, he is not triggering his own breaths, and he is on Volume Assist control ventilation with a decelerating ramp waveform
Question 11
Question
57 y/o F w/ hx of UIP with progressive dyspnea, now on 3L home O2, presents with low grade fever, worsening cough with minimal sputum production and hypoxemia with sats 84% on RA, 91% on 15L oxymask. Wt: 112 kg, ht: 5’5”. Vitals: temp: 38.6 C, RR: 30, HR: 134, BP: 90/55, MAP: 67. Her ABG shows: pH: 7.33/40/72/22/90% on ~80% FiO2. Pt is intubated and started on mechanical ventilation due to hypoxia.
As her physician, you must decide what ventilator settings to commence. Of note, she has evidence of mild to moderate honeycombing at the lung bases and evidence of diffuse bilateral ground glass patchy opacities. She fits criteria for restrictive lung disease with an FVC 57% normal and an FEV1/FVC ratio of 83%. Her DLCO is 48% predicted and her TLC is 62% predicted from PFTs more than 1 year prior.
Please select the most appropriate initial ventilation strategy for this patient.
Answer
-
Synchronized Intermittent Mandatory Ventilation with f: 12, Vt: 500mL, PS: 20, PEEP:14, FiO2: 100%
-
Volume Assist Control with f: 18, Vt: 300 mL, Flow: 80 L/min, PEEP: 5, FiO2: 100%
-
Pressure Support Ventialtion with PS: 24, PEEP: 10, FiO2: 100% with Vt ~ 510-520 mL/breath
-
Volume Assist Control with f: 18, Vt: 450, Flow 60L/min, PEEP: 10, FiO2: 100%
-
Pressure Assist Control Ventilation with Pinsp: 20, PEEP:8, f: 22, FiO2: 100%, I time: 2 sec, ~ Vt 400-420 mL/breath
Question 12
Question
Which of the below images shows a stress index below optimal recruitment?
Answer
-
See Image
-
See Image
-
See Image
{kind=link}
{kind=link}
{kind=link}
Question 13
Question
Your patient has returned from CT scanner and is noted to be more hypoxic than when he left the unit (sats decreasing from 94% on 40% FiO2 to 86-88% on 40%). You check a peak pressure which is increased from 28 to 34. Additionally, his plateau has increased from 24 to 30. Which of the below scenarios is most likely?
Answer
-
Increased secretions requiring suctioning but no evidence of lobar collapse from mucus plugging
-
The ventilator tubing has been partially obstructed during transfer
-
The patient’s ETT has migrated causing Right mainstem intubation
-
The patient’s ETT cuff has ruptured and the tube has migrated above the vocal cords
-
The ventilator has accumulated water in the tubing circuit
Question 14
Question
You wish to calculate a patient’s plateau pressure. Which set of steps below would allow you to calculate the plateau pressure (once you set the ventilator display to show plateau pressures)?
Answer
-
In Pressure Support mode, minus the mean airway pressure from the peak pressure to get a plateau pressure
-
In Volume Assist Control mode, add an inspiratory pause of 3 seconds to your settings; measure plateau pressure while the patient is initiating breaths
-
In Volume Assist Control mode, during ventilator initiated breaths, press the inspiratory pause button until flow becomes zero and maintains steady state to get a plateau pressure
-
In Volume Assist Control mode, during ventilator initiated breaths, press the expiratory pause button until flow becomes zero and maintains steady state to get a plateau pressure
-
In Pressure Control Ventilation, during patient initiated breaths, press the inspiratory pause button until flow becomes zero and maintains steady state to get a plateau pressure
Question 15
Question
Your patient with a new tracheostomy and PEG placed 2 days prior has had abnormal measurements of peak and plateau pressures when you review records over the last 48 hrs. You note that every shift the patient’s peak and plateau pressures decrease just after the patient has a bath, but increase again at the next check. Which is the most likely etiology for this change from the list below?
Answer
-
The patient begins to cough more frequently post bathing
-
The patient’s abdominal binder is removed during bathing and replaced by the subsequent check
-
The patient has an distal XLT trach tube causing recurrent partial R mainstem intubation with turning to the right side during bathing
-
The patient has significant secretions that cause partial airway obstruction whenever he is moved
-
The patient receives a nebulized breathing treatment after every bath
Question 16
Question
34 y/o female with history of drug abuse is admitted to the cardiac intensive care unit with confusion, chest pain, ST elevation in II, III and aVf with reciprocal depressions in the lateral leads, pulmonary edema and hypertensive emergency with BP if 230/125, MAP 160. Additional vitals: temp: 37.6 C, HR: 125, RR: 26, Sat: 87% on RA. ABG prior to intubation: 7.30, PCO2: 25, PaO2: 66, Bicarb: 18, Sat: 85% on RA. Wt: 60 kg, Ht: 5’3”. The patient was intubated in the ED and is still paralyzed from a dose of rocuronium prior to being taken to the cath lab. As the critical care fellow on call, you are asked to make recommendations for her ventilator settings.
The patient has moderate AKI with a creatinine of 2.6. A CT head does not show evidence of blood although assessment of neurological status is limited due to intubation and sedation. CXR here: diffuse bilateral opacities with small bilateral pleural effusions.
Which of the below ventilator settings would be appropriate?
Answer
-
Pressure Assist Control Ventilation with Pinsp:16, PEEP:8, f: 20, FiO2: 100% with Vt ~ 350mL/breath
-
Volume Assist Control with Vt: 420 mL, f: 20, PEEP: 8, FiO2: 100%
-
Pressure Support Ventilation with PS : 18, PEEP: 8, FiO2: 100% with Vt approx 400 mL/breath
-
Synchronized Intermittent Mandatory Ventilation with Vt: 580 mL, f: 14, PS : 10, PEEP: 8, FiO2: 100%
-
Volume Assist Control with Vt: 320, f: 20, PEEP: 8, FiO2: 100%
Question 17
Question
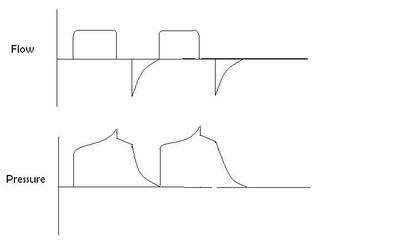
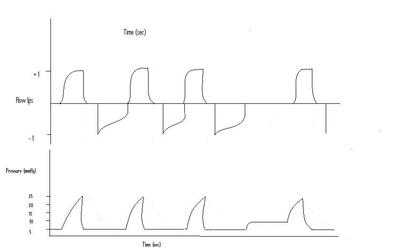
From the above flow and pressure curves, calculated the appropriate AutoPEEP
Image:
autopeep3.JPG (image/JPG)
{kind=link}
Answer
-
2
-
5
-
10
-
15
Question 18
Question
You are walking on rounds getting sign out when you walk by the room of a patient with COPD and left lower lobe pneumonia. You peek inside the room and notice that the patient’s peak pressure is 34. You remember that this patient’s peak pressure was previously 28-30. You enter the room to investigate further. You perform an inspiratory pause maneuver and calculate a plateau pressure of 24. Which of the below scenarios would not cause these changes in peak and plateau pressure?
Answer
-
On exam, you note that the patient is awake and biting on his tube; no bite block is present
-
On exam you note that the patient’s HME is discolored and there is evidence of mucus coating its surface
-
On exam, you note that the patient is receiving a nebulized inhalation therapy through the ventilator
-
On exam, you note that a humidifier has been added to the inspiratory limb of the circuit
-
On exam, you note that the suction catheter is partially obstructing the endotracheal tube.
Question 19
Question
A 49 y/o female with PMHx of severe pneumococcal pneumonia and associated ARDS is on her 12th day of mechanical ventilation. She is being managed on pressure assist-control ventilation with a respiratory rate of 16, PEEP of 8, Inspiratory pressure of 18, Itime: 2secs, FiO2: 40%. On day 12 of mechanical ventilation, it is noted that her average tidal volume size is 360 mL. On day 15, her tidal volume is now an average of 420 mL.
The respiratory therapist comes to tell you that the patient’s tidal volumes are no longer 6mL/kg predicted body weight. What do you do?
Answer
-
Titrate down the Inspiratory Pressure to prevent high tidal volume ventilation
-
Switch the patient to Volume Assist Control and place the patient on strict tidal volumes of 6mL/kg
-
Decrease the inspiratory pressure to minimize volumes, now that the patient’s compliance has worsened
-
Disconnect the patient temporarily from the ventilator to allow escape of air trapping and increased intrinsic PEEP
-
Increase the set respiratory rate so the patient doesn’t have to pull such large volumes to be comfortable
Question 20
Question
78 y/o female is admitted to the neurointensive care unit after suffering from a subarachnoid hemorrhage. Arrangements are made for CTA and interventional radiology. An area of extravasation is noted branching off the R MCA and a coil is placed with resolution. The patient is returned to the ICU for monitoring and blood pressure control. The patient has no evidence of parenchymal blood or intraventricular blood. At this time, the patient’s vitals are: Temp: 37.6, HR: 115, RR: 18, BP: 106/64, MAP of 78, wt: 74 kg, Ht: 5’8”.
Several hours after clipping, the patient is noted to be developing shortness of breath. The patient is currently on oxygen 2L NC but within the next few hours the patient becomes progressively more hypoxic . Her arterial blood gas, on 100% face mask/NRB at 15L is 7.35/35/55/20/sats 88% with a current RR of 25. The decision is made to intubate the patient and place her on mechanical ventilation (paralytics used during intubation).
Additionally, the patient’s BP has decreased and currently is 95/52, MAP of 66. A bedside echo is performed which shows evidence of wall motion abnormalities, apical ballooning and EF of 25%.
Please choose the most appropriate initial ventilator settings for this patient.
Answer
-
Volume Assist Control, Vt: 550, f: 20, PEEP:10, FiO2% 100%
-
Pressure Support ventilation, PS : 15, PEEP:10, FiO2: 100% with estimated tidal volumes ranging from 500-700 ml/breath
-
Volume Assist Control, Vt: 300, f: 16, PEEP: 10, FiO2: 100%
-
Pressure Assist Control, PEEP: 10, Pinsp: 15, f: 16, FiO2: 100% with an estimated Minute Ventilation of: 4 L/min
-
Synchronized Intermittent Mandatory Ventilation, Vol: Vt: 675, f: 16, PEEP: 10, PS: 10, FiO2: 100%
Question 21
Question
After 30 minutes, you obtain an ABG showing pH: 7.56/24/145/24/sat 100%. The patient is triggering her own breaths at a current respiratory rate of 32. The patient’s current ventilator settings are: Volume Assist Control, Vt: 500, f: 18, PEEP: 5 and FiO2: 100%.
What changes to the ventilator would you make at this time?
Answer
-
Increase the PEEP to 15
-
Match the pt’s ventilator RR rate with her own rate by increasing f: 32
-
Lower the FiO2 as tolerated to keep O2 sats > 95% but < 98%
-
Decrease the tidal volume the patient is receiving down to 250 mL
-
Decrease the ventilator rate to 10 breaths per minute
Question 22
Question
What other interventions might you make to prevent the patient becoming more alkalotic?
Answer
-
Give normal saline to cause non-anion gap metabolic acidosis
-
No need to treat, respiratory alkalosis is not harmful
-
Sedate the patient to diminish respiratory drive; if this is not sufficient, consider starting paralysis
-
Give a carbonic anyhdrase inhibitor to interfere with proton losses
-
Continue hyperoxia to blunt the patient’s drive to breathe
Question 23
Question
39 y/o male with morbid obesity presents with obtundation to the ED. He is intubated for airway protection with rocuronium and an ABG is drawn immediately post intubation showing pH: 6.9, PCO2: 120, PaO2: 72, Sat: 91% on 70% FiO2, Bicarb: 38. Vitals post intubation: Wt: 278 kg, Ht: 5’10. Temp: 38.7, HR: 130, RR:12, BP: 98/47, MAP: 64, sat: 92%. Blood cultures, urine cultures, and chest X-ray are done. Empiric antibiotic coverage with pipercillin-tazobactam and vancomycin is started for sepsis. Volume resuscitation is commenced for hypotension.
Which of the following ventilator settings would be appropriate for this paralyzed patient?
Answer
-
Pressure assist control ventilation with Pinsp: 18, PEEP:10, Itime: 2 sec, RR: 15, FiO2: 70%, Vt ~ 550 mL/breath
-
Airway Pressure Release Ventilation: Thigh: 4.1 sec, Tlow: 0.9 sec, Phigh: 25, Plow: 0, PS: 8, FiO2: 70%
-
Volume Assist Control: Vt: 600 mL, f: 26, PEEP: 10, FiO2: 70%
-
Pressure Support ventilation with PS : 16, PEEP:10, FiO2: 70%, Vt ~ 650 mL/breath
-
Synchronized Intermittent Mandatory Ventilation: Vt: 750 mL, f: 22, PEEP: 10, PS: 10, FiO2: 70%
Question 24
Question
The patient has improved clearance of CO2 with a repeat ABG in 1 hr of pH: 7.32/71/112/37/Sat: 98% on ventilator settings of Volume Assist Control: Vt: 580, f: 24, PEEP: 10, FiO2: 70%.
5 hours later you are examining the patient, you notice that the patient’s peak pressures on the ventilator screen are ranging from 35-38. You decide to check a plateau pressure which is 34.
What is your next step in deciding what to do with this patient?
Answer
-
Decrease the patient’s tidal volume to 350 or lower to decrease plateau pressure below 30
-
Measure a bladder pressure
-
Place an esophageal manometer to measure the change in transthoracic pressure with each breath
-
Decrease the patient’s respiratory rate to 15 to decrease the risk of autoPEEP
-
Since the patient’s PEEP is 10 and static compliance is: Vt/Pplat-PEEP, thus the effective plateau is 24 and nothing further needs to be done
Question 25
Question
The transthoracic (trans respiratory system) pressure (34 mmHg) minus transpleural pressure (6mmHg) confirms a transpulmonary pressure of 28mmHg.
Over the next 6 hrs, however, the patient worsens with elevation of alkaline phosphatase, bilirubin and transaminases. You order an US of the liver and CT scan with IV contrast of the abdomen. Your tests show evidence of cholangitis with secondary gall stone pancreatitis. You begin aggressive hydration for pancreatitis, vasopressor support and continue symptomatic care of the patient.
Over the next 4 hours, you notice worsening hypoxia (10 hrs post intubation). Your plateau pressure has increased from 34 to an average of 40, with peak pressures increasing from 38 to 45. Your chest X-ray notes bilateral GGO with a moderate pleural effusion on the left. An ABG is performed which shows a pH: 7.21/72/63/20/Sat: 88% on FiO2: 100%. Current Vent settings are: Volume Assist Control: Vt: 550, f: 18, PEEP: 15, FiO2: 100%. Vitals are: temp: 38.7, RR: 30, HR: 136, BP: 84/42, MAP:56 with sats: 86%.
Which of these below causes would NOT be within the differential diagnosis?
Answer
-
Abdominal compartment syndrome secondary to volume resuscitation and pancreatitis
-
Development of pulmonary edema with occult heart failure
-
Progressive pneumothorax post placement of Internal Jugular central venous catheter
-
Development of ARDS secondary to pancreatitis
-
Bronchospasm due to anaphylaxis from pipercillin-tazobactam
Question 26
Question
What ventilator settings would you consider changing at this time (current settings: Volume Assist Control: Vt: 550, f: 18, PEEP: 15, FiO2: 100%. Vitals are: temp: 38.7, RR: 30, HR: 136, BP: 84/42, MAP:56 with sats: 86%. ABG: pH: 7.21/72/63/20/Sat: 88% on FiO2: 100%. Vitals: temp: 38.7, RR: 30, HR: 136, BP: 84/42, MAP:56 with sats: 86%)?
Answer
-
Increase respiratory rate to normalize PCO2 to 40mmHg, thereby preventing worsening of acidosis
-
Change the patient to Airway Pressure Release Ventilation with Thigh 9 sec, Phigh: 35, Tlow: 0.2 sec, Plow:0, PS: 0 and FiO2: 100%
-
Increase ventilator set rate to match patient’s intrinsic respiratory rate to reduce work of breathing
-
Decrease PEEP to 10 due to concerns for elevated mean airway pressure in the setting of shock and autoPEEP
-
Minimize tidal volume to less than 450 while reducing plateau pressure below 36
Question 27
Question
Based on clinical parameters, imaging etc., you define this patient as having severe ARDS. The patient’s abdomen has been opened, thus minimizing the additive effect of worsening chest wall compliance from the patient’s developing abdominal compartment syndrome. The patient is thrombocytopenic with evidence of DIC and has had continual oozing from his surgical site. He continues to have worsening hypoxia over the next 6hrs (Post ARDS ~ 16hrs). His current ventilator settings are: Vt: 410 mL, f: 25, PEEP: 22, FiO2: 100% with vitals: Temp: 37.9, HR: 129, RR: 35, BP: 89/56 with a MAP of 67 on Norepinepherine 0.2mcg/kg/min and Vasopressin 0.4 units/min, Sat: 87%. Plateau pressure is 32, Ppeak is 35. Current ABG shows 7.22/78/52/22/86%.
At this time, what additional therapy is indicated?
Answer
-
Paralyze the patient with cisatricurium (while receiving sedation)
-
Prone the patient
-
Transition the patient to High Frequency Oscillator Ventilation
-
Continue current management without changes
-
Arrange for the patient to be started on ECMO
Question 28
Question
52 y/o male s/p kidney transplant 5 years ago is admitted from the ED for hypoxia, SOB and decreased mental status requiring intubation for airway protection. You get limited information about the patient’s history, only knowing that the patient has had delayed rejection of his kidney and has been receiving high dose steroids for treatment. Per the patient’s family, he has had fever with progressive dry cough for several days. He has been getting progressively worse and went to the ED due to his SOB and concerns for new onset confusion.
In the ED, a chest X-ray was performed showing normal appearing lungs. On admission to the ED, his vitals are: Temp: 38.3, RR: 32, HR: 119, BP: 113/74, MAP: 87, Sat: 72% on RA, ht is 6’1”, Wt: 87kg and his ABG drawn before intubation is: 7.5/20/52/20/70% sat on RA.
The patient is intubated with succinylcholine, etomidate, morphine and versed. The ventilator has been set at: Pressure Assist Control ventilation with Pinsp: 25, f: 18, PEEP:5, FiO2: 100%. After 30 minutes his ABG shows 7.45/28/80/20/94% on 100% FiO2 with a respiratory rate of 23. The patient is started on empiric antibiotics with cefepime and vancomycin, treatment dose bactrim and steroids for potential PJP infection.
Over the course of the next 24 hrs, the patient’s chest X-ray evolves to show bilateral ground glass opacities. Over the next 12 hours, his saturations dip to the low 80s while PEEP is up titrated to 14 on 100% FiO2. The patient’s ABG at this time shows: pH: 7.29/49/53/24/ 83%.
On Pressure Assist Control Ventilation, what do you expect to see happen?
Answer
-
The patient’s tidal volumes will increase as compliance worsens
-
The patient’s tidal volumes will decrease as compliance worsens
-
The patient’s flow will increase as compliance worsens
-
The patient’s Plateau Pressures will decrease as compliance worsens
-
The patient’s Peak Pressures will increase as compliance worsens
Question 29
Question
The patient’s ventilator is showing return volumes of 340-350 mLs.
Please select the appropriate changes that should be made with the ventilator in this situation.
Answer
-
Changed to Volume Assist Control with a set tidal volume of 500 mL, f: 18, PEEP: 18, FiO2: 100%
-
Continue on Pressure Assist Control Ventilation with PInsp: 30, f: 20, PEEP: 18, Itime: 3 sec, FiO2: 100% however set tidal volume alarms to go off if Vt goes above 480
-
Changed to Synchronized Intermittent Mandatory Ventilation with Vt: 460, f: 15, PS: 25, PEEP: 18 and FiO2: 100%
-
Switch to Airway Pressure Release Ventilation with Phigh: 30, Plow: 0, Thigh:2 secs, Tlow: 0.1 secs, PS:0 and FiO2: 100%
-
Continue on Pressure Assist Control Ventilation with Pinsp: 35, f: 25, PEEP 18, Itime 4sec, FiO2: 100% but set Vt alarm to 520ml
Question 30
Question
Your patient is currently on vent settings: Pressure Assist Control Ventilation with Pinsp: 30, f: 18, PEEP: 18, Itime: 3 secs with FiO2: 100%. (tidal volumes ~ 380mL, with minute ventilation of 8.4L) Vitals are Temp: 36.7, RR: 22, HR: 126, BP: 117/69, MAP of 85, sat: 89%.
On day 5 of admission, you are called emergently to the patient’s bedside to evaluate the patient. You are told by the nurse that he was doing fine until he was turned a few minutes ago. Now, his vitals are showing: temp: 36.8, RR: 26, HR: 145, BP: 92/48, MAP: 63, sat: 78% on 100% FiO2. His breath sounds are difficult to appreciate bilaterally but appear absent on the right. The patient is diaphoretic and on percussion you note hyper-resonance on the R side.
What do you do next?
Answer
-
Take the patient off the ventilator and bag mask ventilating with a PEEP valve set at 15 cmH2O (maximum).
-
Place an angiocath at the mid-clavicular line & 2nd intercostals space to relieve a tension pneumothorax
-
Assess Ppeak and Pplateau to determine if this is a change in compliance or resistance
-
Pull the ETT back 1-2cm to assess for improvement in ventilation
-
Order a stat CXR and await their arrival to evaluate for pneumothorax, mucus plug, or mainstem intubation.
Question 31
Question
25 y/o male is in a motor vehicle accident. He was the front passenger and had significant trauma due to side and front impact from a speeding SUV. He is evaluated and treated for his traumatic injuries including hepatic rupture requiring intraabdominal surgery, comminuted left tibial fracture which underwent ORIF, & chestwall contusions. The patient has been stable post-operatively on mechanical ventilation with plateau pressures of 23-24, peak pressures of 26-27, sating 100% on Synchronized Intermittent Mandatory Ventilation, Vt: 550 mL, f: 12, PS: 10, PEEP:8, FiO2: 40% the first 6 hrs post admission. He has central access (subclavian), a neck brace (pt is sedated), closed abdominal incision and his left leg is bandaged and pinned. On the evening of his post-operatively day zero, the RN asks you to come evaluate the patient for hypoxia and peak alarms being triggered. At the bedside the patient is sedated, vitals show: 5’11’, wt: 91kg, temp: 37.6 C, HR: 120 and irregularly irregular, SBP: 105/72 with MAP: 83, RR: 32, pulse ox: 84%. His peak pressure is 33 on controlled breaths.
After increasing the FiO2 to 100%, the O2 saturation improves to 92%. What would you do next to clarify the source of this patient’s acute hypoxemia?
Answer
-
Examine the patient, listen for bilateral breath sounds, check a plateau maneuver
-
Send the patient for an emergent CTA to rule out PE
-
Have the nurse draw blood cultures, sputum and urine cultures while you place the patient on low tidal volume ventilation
-
Silence the Peak alarms – they don’t mean anything and are just annoying
-
Perform an expiratory pause maneuver to determine if autoPEEP is the source
Question 32
Question
You change the patient to Volume Assist Control mode with settings: Vt: 550mL, f: 12, PEEP: 8, FiO2: 100% to provide a saturation of 93%. Pt is sedated to RASS -2 to calm his anxiety and distress.
You decide to assess the patient’s plateau pressure. After confirming plateau pressure will be displayed on the screen, what steps do you take?
Answer
-
You press the expiratory pause button for 5 seconds during breaths with patient effort during inhalation
-
You press the inspiratory pause button only on breaths without patient effort, hold for a minimum of 3 seconds and repeat this up to 3 times to confirm stability
-
You dial in an inspiratory pause of 3 seconds as part of your ventilator settings and record the plateau of the next 3 breaths, without concern for whether the patient has spontaneous effort during inhalation
-
You press the expiratory pause button only on breaths without patient effort, hold for a minimum of 3 seconds and repeat this up to 3 times to confirm stability
-
You press the inspiratory pause button for 5 seconds during breaths with patient effort during inhalation
Question 33
Question
The patient’s plateau pressure is 27 (from 23-24). (Remember: peak pressures: 33 from 26-27)
What is the most likely etiology of the patient’s source of hypoxemia from the below options?
Answer
-
Acute moderate to large pneumothora with lung collapse
-
Movement of the ETT causing incomplete R mainstem intubation
-
Flash pulmonary edema from A. fib with RVR
-
Large mucous plug causing lobar airway collapse
-
ETT cuff with significant airleak
Question 34
Question
On your exam, the patient is noted to have minimally decreased breath sounds on the left. You check a CXR and note that the ETT is at or just below the carina towards the right. You pull back the ETT 3 cm and the patient’s peak pressures decrease back to 27. Over the next few hours you are able to titrate the patient’s FiO2 back to 40%.
Over the next 24 hrs, the patient begins to have increasing sputum production, fevers and is started on antibiotics for a right middle lobe consolidation. His ventilator settings are: Vt: 550mL, RR: 12, PEEP: 8, FiO2: 40% with oxygen saturation 93%. Over the next 12 hours, the patient’s compliance and oxygenation worsen, with the patient requiring PEEP:12, FiO2: 60% to maintain sats > 90%. On these settings, his Peak pressure is 35 and his plateau is 27. The patient has copious, thick secretions.
The night-shift nurse calls you at 2am in the morning because the patient is once again desaturating. Additionally, he has had an increase in his peak pressure to 43. You check his plateau and now it has increased to 35.
Which of the below actions would you take to reduce the patient’s elevated plateau and peak pressures?
Answer
-
Exchange the ETT over a tube exchanger as the ETT is clogged with dried mucus
-
Insert a bite block to prevent the patient blocking his airway
-
Remove the dirty HME from the ventilator circuit as it is causing obstruction of ventilation
-
Suction the patient to remove large mucus plug causing lobar collapse
-
Provide bronchodilators due to presumed bronchoconstriction on the ventilator
Question 35
Question
24 y/o male admitted to the ICU post ingestion of 35 tablets of seroquel. The patient is intubated in the ED for airway protection due to somnolence. Additionally, an OGT was placed and the pt was given 50g of activated charcoal as his ingestion occurred within 30 minutes of arrival to the ED. The patient is transferred to the ICU for monitoring of hemodynamics, cardiac arrhythmias and mental status.
On admission, the patient is on ventilator settings of: Volume Assist Control, Vt: 500, f: 12, PEEP: 5, FiO2: 100%. Vitals are: temp: 36.8 C, RR: 12, HR: 70, BP: 122/78 with MAP: 93, sat: 100%. Wt: 80 kg, ht: 5’6”. ABG shows: pH: 7.28/53/312/26/100% , peak pressure: 22, plateau: 16.
You wean the patient’s FiO2 to keep sats > 92%. Which other change to the ventilator is most appropriate at this time?
Answer
-
Continue Volume Assist Control but decrease tidal volume to 400mL
-
Continue Volume Assist Control but increase f to 18.
-
Change the pt to Synchronized Intermittent Mandatory Ventilation with Vt: 500, f:12, PEEP:5, PS:10
-
Change the pt to Pressure Assist Control Ventilation with Pinsp: 20, PEEP:5, f: 12, Itime: 3 secs with an approximate Vt: 500mL to reduce dyssynchrony
-
Place the pt on Pressure Support Ventilation with PS : 12, PEEP: 5
Question 36
Question
The patient is waking up and begins triggering his breaths at a rate of 23-25 bpm. He is saturating 100% on 30% FiO2. On exam, breath sounds are clear without evidence of wheezes, rhonchi or rales.
Which scenario suggests the patient is stable for extubation?
Answer
-
The patient withdraws to stimulation in his lower extremities, does not open his eyes or follow command, has a positive cough and gag reflex. He is placed on a Pressure Support trial of 5/5 for 30 minutes and his tidal volumes are 250 with a respiratory rate of 42.
-
The patient is only responsive to severe pain, he has no cough but + gag reflex. He is placed on a Pressure Support trial of 5/5 for 30 minutes and his tidal volumes are 500 with a respiratory rate of 18.
-
The patient follows all commands, raises his head off the bed, has a + cough and gag. He is placed on a Pressure Support trial of 5/5 for 30 minutes and his tidal voThe patient follows all commands, raises his head off the bed, has a + cough and gag. He is placed on a Pressure Support trial of 5/5 for 30 minutes and his tidal volumes are 150 with a respiratory rate of 18.
-
The patient follows all commands, raises his head off the bed, has a + cough and gag. He is placed on a Pressure Support trial of 10/10 for 30 minutes and his tidal volumes are 400 with a respiratory rate of 18.
-
The patient withdraws to stimulation in his lower extremities, does not open his eyes but follows commands including lifting his head, has a positive cough and gag reflex. He is placed on a Pressure Support trial of 5/5 for 30 minutes and his tidal volumes are 300 with a respiratory rate of 18.
Question 37
Question
A 76 y/o M with PMHx of tobacco use for > 45 pack years, hx of severe COPD with FEV1 42% predicted presents to the ED with low grade fever, cough with increased sputum production, SOB and hypoxia. On exam, the patient has poor air entry and pronounced end expiratory coarse polyphonic wheezes at the bases. His vitals are: temp: 38.2, RR: 34, SBP: 146/97, MAP: 113, HR: 123, Sat: 90% on 8L NC. Wt: 50kgs, ht: 5’10”. Pt is anxious, cannot speak 2 words without having to pause to breathe, mildly diaphoretic and complaining of chest tightness. CXR is clear with hyperinflation. An ABG is done which shows: 7.31/56/78/30/sat: 92%. You try to calm the patient and treat with BiPAP ventilation but the pt complains of claustrophobia and PTSD. You treat with inhaled beta-agonists and ipratropium, steroids and azithromycin. However, the patient does not improve, his vitals change with temp: 37.9, RR: 41, HR: 133, BP: 102/43, MAP: 63, sat: 87%. You get an ABG (7.22/73/65/30/sat: 86%) and the patient is intubated for impending respiratory failure with versed, fentanyl and rocuronium.
Which of the below ventilator settings would be appropriate to initiate at this time?
Answer
-
Pressure Support ventilation with PS : 18, PEEP: 5, FiO2: 100% with Vt ~ 475mL/breath
-
Volume Assist Control with Vt: 575mL, f: 13, flow of 100L/min, PEEP: 5, FiO2: 100%
-
Synchronized Intermittent Mandatory Ventilation with Vt: 650 mL, flow 80 L/min, f: 12, PEEP: 5, PS: 10, FiO2: 100%
-
Pressure Assist Control Ventilation with Pinsp: 18, PEEP: 5, Insp time: 2 sec, f: 20, FiO2: 100% with ~ Vt: 600mL
-
Volume Assist Control with Vt: 550, f: 25, flow of 100 L/min, PEEP: 5, FiO2 : 100%
Question 38
Question
The patient’s blood pressure improves over the next hour back to 147/79, MAP: 102.
Which aspect of the process of intubation and mechanical ventilation caused the patient’s blood pressure to improve?
Answer
-
Positive pressure ventilation improves cardiac output by increasing preload.
-
Sedation promotes improved exhalation and thereby decreasing intrathoracic pressure.
-
Sympathetic stimulation from intubation caused resolution of the patient’s hypotension.
-
Positive pressure ventilation increases afterload and systemic venous resistance.
-
Improved aeration with mechanical ventilation reduces pulmonary vasoconstriction and thereby reduces end diastolic volume.
Question 39
Question
A 57 y/o M with ESLD presents intubated for airway protection after large volume hematemesis in the field. He is stabilized with blood products and placement of a Blakemore tube prior to receiving emergent TIPS . The patient returns from IR on the ventilator. His current vitals show: temp: 36.3 C, HR: 121, RR: 18, BP: 91/51, MAP 64 on 0.1 mcg/kg/min of Norepinepherine. Wt: 80 kgs; ht: 5’9”. His ventilator is set on Volume Assist Control with Vt: 560mL, f: 16, PEEP: 5, FiO2: 50%. His current ABG shows: 7.3/39/121/18/96%. The patient’s current Hgb: 8.6.
Over the course of the next 12 hrs, the patient appears to be improving hemodynamically and is weaned off Norepinepherine. Sedation has been minimized but there is significant evidence of confusion and encephalopathy. The patient is triggering all his own breaths at a rate of ~ 19 breaths per min. He has minimal secretions. He has a positive gag and a cough, but cannot follow any commands.
Which of the below scenarios regarding mechanical ventilation would you choose for your patient at this time?
Answer
-
Transition the patient to Synchronized Intermittent Mandatory Ventilation with Vt: 560, f:12, PS: 15, PEEP:5, FiO2: 40%
-
Transition the patient to Pressure Support Ventilation with PS: 12, PEEP:5, FiO2: 40% to keep Vt: 300-350 mL/breath
-
Transition to Pressure Assist Control Ventilation with Pinsp: 15, PEEP:5, f: 20, I time: 3 sec, FiO2:40% with Vt: 450-460 mL/breath
-
Transition the patient to Pressure Support Ventilation with PS: 19, PEEP:5, FiO2: 40% to keep Vt: ~ 475-500 mL/breath
-
Perform an SBT; if the patient’s rapid shallow breathing index is below 120 at 30 minutes, extubate the patient.
Question 40
Question
The patient has been doing well and is currently on Pressure Support Ventilation with PS: 11, PEEP:5, & FiO2: 28%. A spontaneous breathing trial is performed on PS 5/PEEP 5.
Which of the selections below would make you comfortable to proceed with extubating the patient?
Answer
-
Pt is Sitting up in bed, intermittently agitated but eyes open, tracking, mostly following commands, + cough and gag, minimal secretions, 5 minute RSBI of 40, 30 minute RSBI of 80.
-
Pt is Somnolent, responds to pain and touch, intermittently to voice, not following commands, + cough and gag, minimal secretions, RSBI at 5 min: 45, 30 min: 90.
-
Pt is Awake, alert, following commands, + cough, + gag, requiring suctioning every 1 hr with thick secretions, RSBI at 5 min: 60, RSBI at 30 min: 90
-
Pt is Awake, following commands but agitated. Gesticulating that he wants the tube removed. + cough, gag, scant secretions, elevates head off the bed. RSBI at 5 minutes: 120, unable to tolerate 30 minute due to RR > 40.
-
Awake, comfortable on vent, following all commands, + cough and gag, minimal secretions. RSBI at 5 min: 90, at 30 minutes: 170
Question 41
Question
A 67 y/o female is transferred from an outside hospital for failure to wean from the ventilator. On your review of her history, you note that she was initially admitted for septic shock secondary to E. coli bacteremia and UTI (1 week ago). She was intubated on the second day of her admission to the OSH after developing hypoxemic respiratory failure which was later diagnosed as ARDS. The patient was in renal failure, as well, and continues to receive HD daily for diuresis. She is now 6 days post intubation. She has received appropriate antibiotics, steroids for her shock and ARDs. She did not receive paralytics and was not proned during the course of her OSH hospitalization. She has been off vasopressor support for > 48hrs. Her current vitals are: temp: 37.1, RR: 23, HR: 87, BP: 143/86, MAP: 105, Sat: 97%, wt: 52kg, Ht: 5’4” on vent settings Volume Assist Control with Vt: 320mL, f: 18, PEEP: 15, FiO2: 50% with an ABG showing: pH: 7.28/49/114/18/ Sat: 98%. Ppeak: 23, Pplat: 20.
What ventilator changes would you make at this time?
Answer
-
Decrease FiO2 to 30% as patient is not a candidate for extubation while FiO2 is > 30%
-
Decrease the patient’s respiratory rate to allow for permissive hypercapnea.
-
Decrease the PEEP as the patient is no longer significantly hypoxic on a FiO2 of only 50%.
-
Increase the patient’s tidal volume to improve CO2 clearance
-
Start daily spontaneous breathing trials without changing current ventilator settings between trials
Question 42
Question
Over the next 2 days, the patient slowly improves and she is weaned down to PEEP 10 with FIO2 50%. You decide to extubate the patient and perform a spontaneous breathing trial.
Which of the below components is NOT recommended when performing an SBT?
Answer
-
Holding patient sedation or limiting sedation to keep the patient awake but not anxious
-
Performing a breathing trial for a minimum of 30 minutes
-
Making sure that the patient doesn’t have a contraindication for extubation, such as post-reconstructive tracheal surgery or obtundation
-
Checking a cuff leak on all patients
-
Placing the patient on the T-piece trial with no ventilator support (only oxygen flow)
Question 43
Question
The patient failed her SBT at this time, however, she is awake and breathing on her own. She appears uncomfortable on the ventilator so you decide to transition her to Pressure Support Ventilation.
Which factor should you consider in transitioning the patient to Pressure Support Ventilation?
Answer
-
In Pressure Support Ventilation, if the patient’s tidal volumes are < 200, consider increasing the patient’s PEEP
-
The practitioner is required to titrate the Pressure Support to provide a tidal volume sufficient to clear CO2 from the patient’s alveoli (ventilation > dead space)
-
If the patient has a RR >30 on controlled ventilation, he/she will not tolerate Pressure Support Ventilation
-
If the patient is hypoxic, requiring more than 50% FiO2 or PEEP > 8, Pressure Support Ventilation is contraindicated
-
If your patient’s intrinsic RR < 10, Pressure Support Ventilation is contraindicated as the patient will be at risk of hypercarbic respiratory failure
Want to create your own Quizzes for free with GoConqr? Learn more.