6164771
Description
Flashcards by Ashutosh Kumar, updated more than 1 year ago
|
|
Created by Ashutosh Kumar
over 8 years ago
|
|
| Question | Answer |
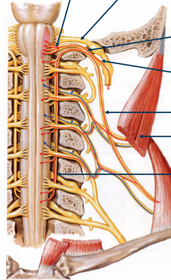
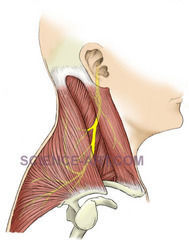
| Name Origin: Course: Innervates: | Accessory nerve Origin: The accessory nerve (cranial nerve 11), has a cranial root and a spinal root. The cranial root arises from the nucleus ambiguus at the level of the open medulla. The spinal root arises from the cell bodies in the posterolateral aspect of the ventral horn of grey matter C1-C5; called the spinal accessory nucleus. The spinal root will enter the cranium via the foramen magnum and will then intermingle with the cranial roots of 11 in the jugular foramen as they exit the cranium. They separate after they exit the jugular foramen; the cranial root will travel with the vagus nerve whereas the spinal root will travel to innervate the sternocleidomastoid and trapezius. |
| Name Origin: Course: UMN lesion effect and why: | Spinal part of accessory nerve Origin: The accessory nerve (cranial nerve 11), has a cranial root and a spinal root. Origin: The spinal root arises from the cell bodies in the posterolateral aspect of the ventral horn of grey matter C1-C5; called the spinal accessory nucleus. Course: The spinal root will enter the cranium via the foramen magnum and will then intermingle with the cranial roots of 11 in the jugular foramen as they exit the cranium. They will then separate after they exit the jugular foramen. The spinal root is will emerge onto the neck just superior to the middle of the posterior border of the sternocleidomastoid muscle. UMN lesion: The spinal accessory nucleus can be subdivided into two parts; C1 and C2 supply the sternocleidomastoid whereas C3 and C4 supply the trapezius. C1 and C2 receive bilateral UMN innervation from the primary motor cortex. Hence, an UMN lesion causes contralateral weakness of the trapezius but relative sparing of the sternocleidomastoid. |
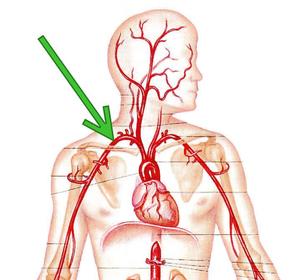
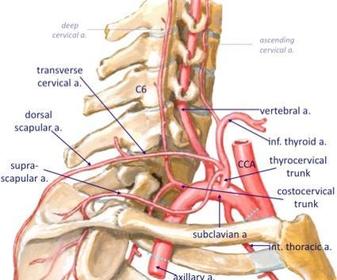
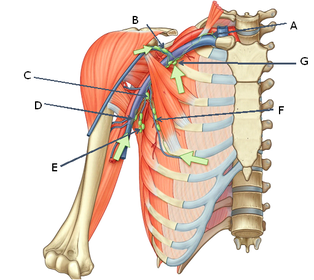
| Name Origin on the right and left side: First 3 branches: | Subclavian artery Origin: Right subclavian artery arises from the brachiocephalic trunk. Origin: Left subclavian artery arises as the 3rd branch of the aortic arch. On both sides, the first 3 branches are: Thyrocervical trunk. Internal thoracic artery. Vertebral artery. |
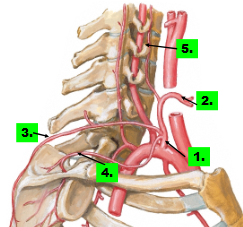
| Names of all Course of 1, 2 and 5: | The thyrocervical trunk (1) arises medial to the scalenus anterior muscle and has 3 branches: Suprascapular artery (4). Transverse cervical artery (3). Inferior thyroid artery (2); the largest and most important branch which supplies the inferior pole of the thyroid gland. The vertebral artery (5) will run in the transverse foramina from C6-C1 and supply the brainstem and brain. |
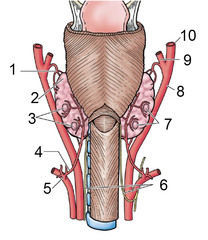
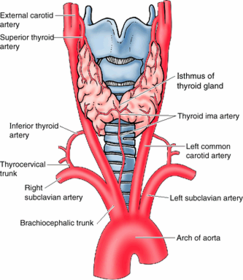
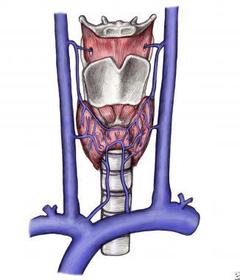
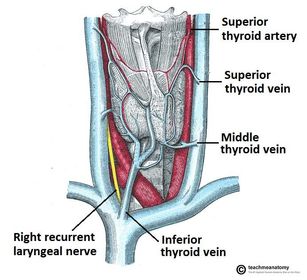
| Thyroid gland arterial supply | Thyroid gland arterial supply Superior thyroid artery (1): arises as either the first or second branch of the external carotid artery. It is the first anterior branch of the external carotid artery and travels deep to the infrahyoid muscles to supply the superior pole of the thyroid gland. Inferior thyroid artery (4): Arises as the largest and most important of the 3 branches of the thyrocervical trunk (5) and travels to supply the inferior pole of the thyroid gland. |
| Thyroid gland venous drainage | Thyroid gland venous drainage Superior and middle thyroid veins: drain into the internal jugular vein (along with the tributaries; inferior petrosal sinus, facial vein, lingual vein and pharyngeal vein). Inferior thyroid veins: drain into the brachiocephalic veins. |
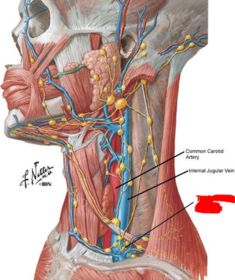
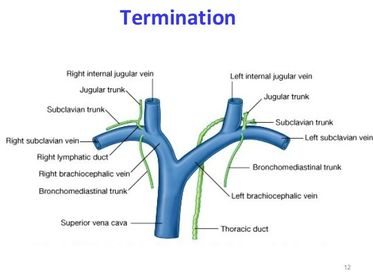
| Name Termination: | The thoracic duct Termination: Drains into the junction of the left internal jugular and left subclavian veins. |
| Name A Termination: | The right lymphatic duct Termination: Drains into the junction of the right internal jugular and right subclavian veins. |
| Name Relation to carotid sheath: Origin and course: Supplies (4): | Cervical sympathetic trunk Relation: Lies posterior to the carotid sheath embedded in the prevertebral fascia. Course: The sympathetic neurons from T1 enter the sympathetic chain and synapse at the superior cervical ganglion. The postganglionic fibres follow the internal carotid to the ophthalmic artery. They are distributed by passing through the ciliary ganglion and short ciliary nerve, innervating the dilator pupillae muscle (dilation of pupil), superior tarsal muscle (smooth muscle found inferiorly), sweat glands and blood vessels. |
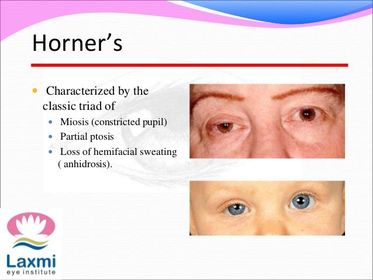
| Name Syndrome and 4 clinical signs of damage: | Cervical sympathetic trunk Effects of damage: ipsilateral Horner’s syndrome, with 4 clinical signs: Miosis (abnormal constriction of the pupil); Loss of sympathetic innervation of the dilator pupillae muscle. Mild ptosis: Loss of sympathetic innervation of the superior tarsal muscle (smooth muscle found inferiorly). Loss of heat induced sweating. Loss of heat induced or emotional vasodilation. |
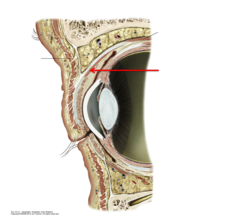
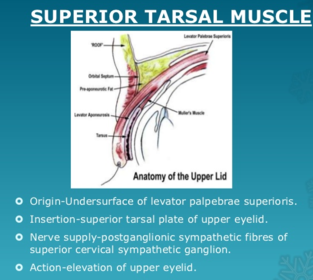
| Name Function: Innervation: Effect of LMN lesion and why: | Superior tarsal muscle Function: Raise eyelids Innervation: Post ganglionic sympathetic fibres from the superior cervical ganglion Effect of LMN lesion and why: Partial ptosis since innervation of levator palpebrae superioris is via the oculomotor nerve (cranial nerve 3) and is intact, so it can raise the eyelid partially. |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Want to create your own Flashcards for free with GoConqr? Learn more.