Description
|
|
Created by sophietevans
about 11 years ago
|
|
Page 1
{kind=link}
{kind=link}
{kind=link}
1
2
3
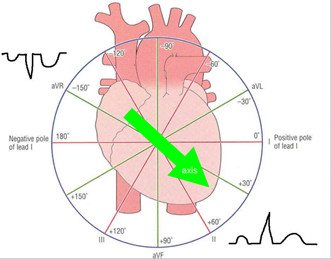
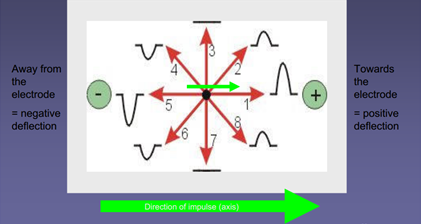
The electrocardiogram and mean cardiac vector (23/09/13 prac) Excitation-contraction coupling forms the basis of the importance of the ECG. Individual cells (primarily in the sinoatrial node) can generate action potentials which are propagated directly and rapidly between cardiac cells via intercalated discs (gap junctions). The action potential a cell undergoes is accompanied by an influx of Ca2+ ions, which results in contraction by the same sliding filament mechanism as skeletal muscle. This means that examining the electrical activity of the heart can tell us a lot about its mechanical effectiveness. Even though the electrical activity of individual cardiac muscle cells is tiny, the fact that millions of them are undergoing action potentials in a co-ordinated fashion (a functional syncytium) means that there are fairly large electrical changes occurring in the chest cavity. These can be recorded as voltages on the surface of the body between suitably placed electrodes. What are electrocardiograms used for? An ECG shows how fast your heart is beating (e.g. may show brachycardia in hypothermia), whether the rhythm of your heartbeat is steady or irregular (this could suggest that a part of the heart is not conducting properly, or that the sinoatrial node is out of rhythm), and the strength and timing of electrical signals as they pass through the heart (this could help locate areas of decreased function, e.g. in a myocardial infarction). P – depolarising electrical activity in the atria (atrial systole) QRS – depolarising electrical activity in the ventricles (ventricular systole) T – repolarising electrical activity in the ventricles (ventricular diastole) We attached 3 leads (each a pair of recording electrodes) to each subject (1: right arm and left arm; 2: right arm and left leg; 3: left arm and right leg), as well as an ‘earth/reference’ electrode to the right leg, and recorded 5 beats at 25 mm/s for both normal, quiet breathing and for breath holding. This meant that: the right arm had 2 negative electrodes, the left arm had 1 negative and 1 positive electrode, and the left leg had 2 positive electrodes. Einthoven’s triangle is used to calculate the mean cardiac vector (the overall direction and magnitude of the heart’s electrical activity during systole). If an electrical impulse travels towards a positive electrode, there will be a positive (upwards) deflection of the trace from the baseline (image 1). If an electrical impulse travels towards a negative electrode, there will be a negative (downwards) deflection of the trace from the baseline. Further, if an electrical impulse travels towards an electrode there will be a positive deflection from the baseline, and if an electrical impulse travels away from an electrode there will be a positive deflection from the baseline (image 2). SO the deflections from each electrode tell us which angle of the heart we are ‘looking’ at (given that we know the electrical activity starts in the sinoatrial node of the right atrium and travels through the atria and then the ventricles. We measured the maximum positive and negative deflections of the QRS complex (as ventricular depolarisation is of large magnitude and is highly directional) for each lead in mm, and then calculated the overall mean activity during the QRS complex (e.g. +8mm plus -3mm = +5mm). We then converted this to mV (1 mV = 10mm deflection) and plotted these values on Einthoven’s equilateral triangle. Zero degrees and the plus and minus directions were indicated on the sheet. We drew perpendicular lines through the mV value for each lead and these lines joined up to form a small triangle. The angle between the centre point of this triangle and the 0° point was the vector angle (normal range = -30° and +90°). The size of the vector was the distance between the centre of Einthoven’s triangle, and the centre of the triangle produced by drawing the perpendicular lines to the voltage values for each lead. Class data: · Using an unpaired T-test, there was no evidence for a difference in size or angle of the mean cardiac vector in males and females. However, there was strong evidence for a difference in mean height of a person and whether they were male or female. The lack of difference for the mean cardiac vector may have been because the diagram of Einthoven’s triangle was not particularly accurate. · Using a paired T-test, there was no evidence for a difference between normal vector size and breath-holding vector size, and normal vector angle and breath-holding vector angle. One would expect the vector angle to change as our hearts deviate to the side during inhalation, so the diagram used to work out the angles is not likely to have been accurate enough. (My data: normal vector angle = +78°, breath-holding vector angle = +85°). An axis between -30° and -90° is a left axis deviation, which can be caused by ventricular tachycardia, inferior myocardial infarction, left ventricular hypertrophy, or left anterior hemiblock. An axis between +120° and +180° is a right axis deviation, which can be caused by right ventricular hypertrophy (e.g. in fibrosis of lung tissue as more blood has to be pumped to be oxygenated and it is against more resistance), anterolateral myocardial infarction, or left posterior hemiblock. An axis between -90° and +180° is an extreme axis deviation, which can be caused by ventricular tachycardia, emphysema, and a pacemaker (image 3).
New Page
Want to create your own Notes for free with GoConqr? Learn more.