3094701
Description
Mind Map by wallacejr@hotmail.co, updated more than 1 year ago
|
|
Created by wallacejr@hotmail.co
over 9 years ago
|
|
PHARMACOLOGY BLOCK 2 : CNS & PAIN
- caution... serotonin
syndrome .; • Mild to
life threatening –
Cognitive‐ agitation,
restlessness,
hypomania,
confusion –
Autonomic‐
hyperthermia,
hypertension,
tachycardia –
Neuromuscular‐
tremor, ataxia,
hypertonia
- neurotransmitters function and illness
- Noradrenaline (NA)
- Dopamine (D)
- Serotonin
5-hydroxytryptamine
(5-HT)
- Acetylcholine
- Gamma-amino
butyric acid (GABA)
- Glutamate
- Memory, learning
- Alzheimers, stroke,
huntingtons,
epilepsy
- Alzheimers, stroke,
huntingtons,
epilepsy
- Memory, learning
- Motor control, memory,
consciousness
- Anxiety, insomnia,
aberrant behaviour,
epilepsy
- Anxiety, insomnia,
aberrant behaviour,
epilepsy
- Glutamate
- Cognition, skeletal
muscle movement,
memory, consciousness
- Parkinson
disease, dementia
- Parkinson
disease, dementia
- Gamma-amino
butyric acid (GABA)
- As for NA plus
behaviour, pain
transmission, emesis
- Depression, ADD,
headaches, eating
disorders, insomnia;
vomiting
- Depression, ADD,
headaches, eating
disorders, insomnia;
vomiting
- Acetylcholine
- Skeletal muscle
movement, behaviour,
emesis, hormone
release
- Parkinson disease,
schizophrenia,
aberrant behaviour,
psychoses; emesis
- Parkinson disease,
schizophrenia,
aberrant behaviour,
psychoses; emesis
- Serotonin
5-hydroxytryptamine
(5-HT)
- Arousal, sleep, mood,
appetite, hormone release,
body temp
- Depression, insomnia,
eating disorders,
narcolepsy, ADD
- Depression, insomnia,
eating disorders,
narcolepsy, ADD
- Dopamine (D)
- illness occurs because imbalanced
- to much; over excite neuron or ^ in
receptors or transmitters or
activity
- to little; neurons not excited or - receptors transmitters or activity
- examples: depression...low
serotonin and noradrenaline;
anxiety insomnia... high glutamate
low gaba low serotonin;
- to much; over excite neuron or ^ in
receptors or transmitters or
activity
- Noradrenaline (NA)
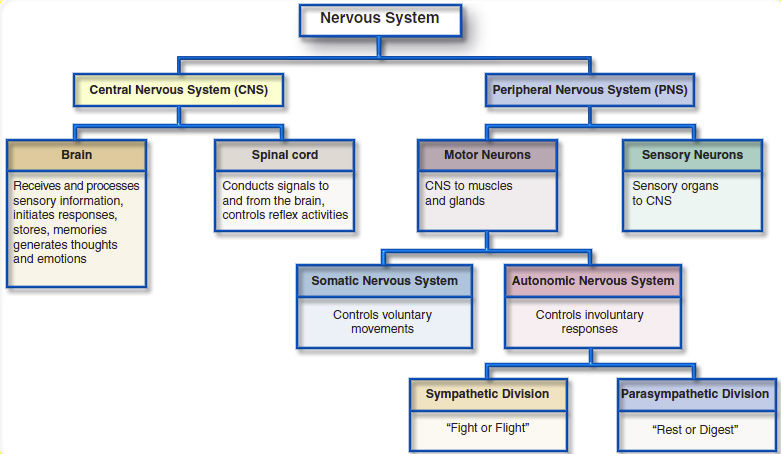
- CNS CONTROLS input AND output in diffrent areas of brain
- RETICULAR ACTIVATING SYSTEM: arousal;pain;consciousness;muscle tone
- LIMBIS SYSTEM: expressed emotions; behavoural; perseptions learning and memory
- EXTRAPYRAMIDAL SYSTEM; innervation of muscles limbs head and eyes
- BASAL GANGLIA; voluntary movements
- BASAL GANGLIA; voluntary movements
- EXTRAPYRAMIDAL SYSTEM; innervation of muscles limbs head and eyes
- LIMBIS SYSTEM: expressed emotions; behavoural; perseptions learning and memory
- RETICULAR ACTIVATING SYSTEM: arousal;pain;consciousness;muscle tone
- antidepressants
- antipsychotics
- anxiolytics
- mood stabillisers
- antiepileptics
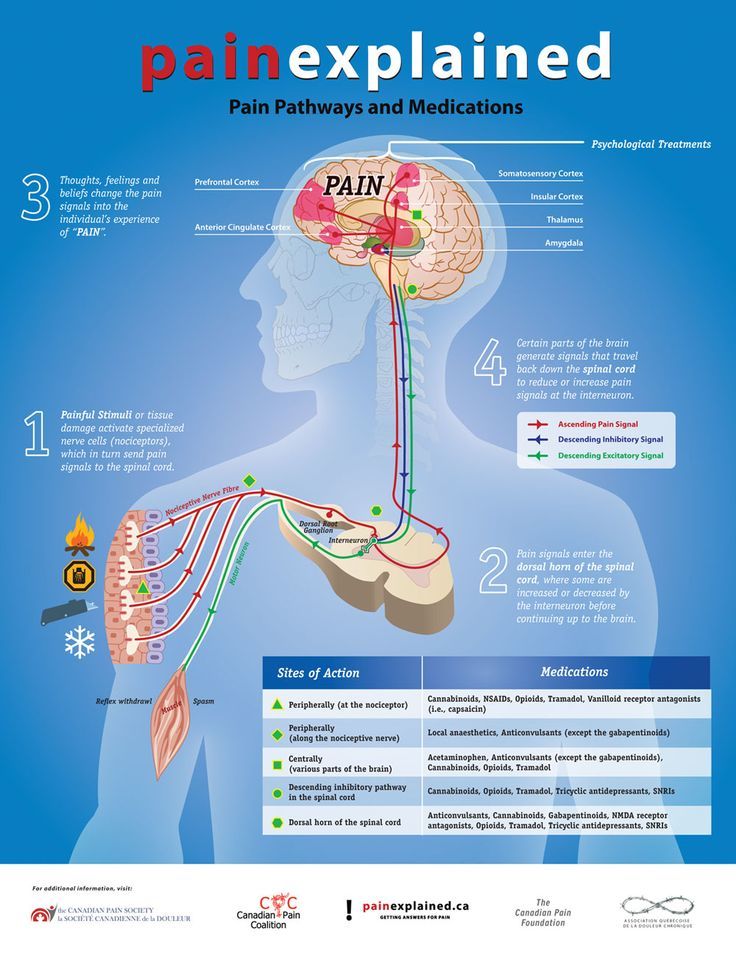
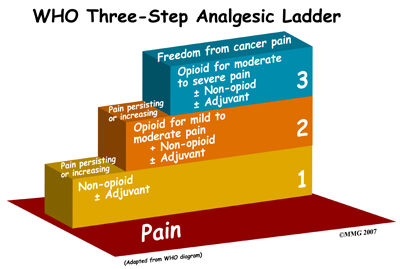
- pain
- control or relive pain
- Narcotic-opium (morphine/codeine/ pethidine/fentanyl) bind to opioid receptors stop subtance p .
liver high pass effect lwr dose result. kidney and bile out. Paracetamol, COX-2 inhibitors and NSAIDs
are PG synthesis inhibitors • Paracetamol – unknown what enzyme/s are inhibited • COX-2 inhibitors
– inhibits cyclooxgenase 2 enzyme (COX-2) • NSAIDs – inhibits cyclooxgenase enzymes (COX-1
BALANCING and COX-2 PROTECTIVE) GENRAL • nitrous oxide • isoflurane • desflurane •
sevoflurane • propofol • thiopentone (Pentothal) LOCAL• lignocaine (Xylocaine) • amethocaine • bupivacaine
• cocaine BLOCK PAIN
- Narcotic: mimic natural peptides in our bodies (endorphins) • The effects of narcotic from therapeutic to overdose
includes analgesia, sedation, hypnosis, coma and finally death** benzos... • Morphine ‐ short half life (4 hrs) so dosing
has to be frequent; tolerance develops • Pethidine – used in child birth and surgery for mild to severe pain ‐ causes
less respiratory depression than morphine ‐ does not cause constipation. • Codeine • Fentanyl epidural (intrathecal)
transdermal patch (Duragesic®) lollipop (Actiq®) • Tramadol • Methadone ‐ used as a substitute for morphine and
heroin addiction as has lesser withdrawal symptoms ‐ 24 hrs half life ‐ strong analgesic NSAIDS AND COX2 -nausea,
vomiting, ulcerations, and headache AND gi. PARACETAMOL- metabolised in the liver and can cause hepatotoxicity
(alcoholics especially).
- • GENRAL Depress the CNS, ease pain and cause loss of consciousness (in most instances). • IV or
inhalation • Used in major surgery. Examples: N2O, flurane gases, propofol LOCAL: • Block pain at site
where drug administered • Allows consciousness to be maintained • Administration route: topical,
intradermal, subcutaneous, epidural, intrathecal, intravenous. • Uses: dental surgery; suturing of
skin lacerations; minor surgery at a localised area; epidural Examples: lignocaine; amethocaine;
bupivicaine
- Adverse Effects of General Anaesthetics • CV – drop in blood pressure • CNS – respiratory depression
• Liver – “Halothane Hepatitis” • Uterus – relaxes uterine muscles • Malignant Hyperthermia – rare •
CTZ ‐ Nausea/vomiting. local 1. Local anaesthetics can also affect sodium channels in other parts of
the body e.g. heart. This can lead to an abnormal heart beat. 2. Epidural anaesthetic could introduce
foreign substances into the CSF. 3. Overdosage of local anaesthetic could lead to dosedependent CNS
side effects; insomnia, visual and auditory disturbances, convulsions, shivering and CNS stimulation.
4. The ester containing local anaesthetics can cause allergic reactions.
- Adverse Effects of General Anaesthetics • CV – drop in blood pressure • CNS – respiratory depression
• Liver – “Halothane Hepatitis” • Uterus – relaxes uterine muscles • Malignant Hyperthermia – rare •
CTZ ‐ Nausea/vomiting. local 1. Local anaesthetics can also affect sodium channels in other parts of
the body e.g. heart. This can lead to an abnormal heart beat. 2. Epidural anaesthetic could introduce
foreign substances into the CSF. 3. Overdosage of local anaesthetic could lead to dosedependent CNS
side effects; insomnia, visual and auditory disturbances, convulsions, shivering and CNS stimulation.
4. The ester containing local anaesthetics can cause allergic reactions.
- all addictive and abuseive
- Monitoring and Care Associated with General and Local
Anaesthetics 1. Make sure vital signs and consciousness are
monitored before, during and after general anaesthetic use. 2.
Use narcotics sparingly while client is attempting to regain
consciousness. 3. Monitor vital signs and conscious state regularly.
Local anaesthetics can cause cardiac depression and CNS
stimulation. 4. Evaluate local anaesthetised areas for sensation
and movement.
- Monitoring and Care Associated with General and Local
Anaesthetics 1. Make sure vital signs and consciousness are
monitored before, during and after general anaesthetic use. 2.
Use narcotics sparingly while client is attempting to regain
consciousness. 3. Monitor vital signs and conscious state regularly.
Local anaesthetics can cause cardiac depression and CNS
stimulation. 4. Evaluate local anaesthetised areas for sensation
and movement.
- • GENRAL Depress the CNS, ease pain and cause loss of consciousness (in most instances). • IV or
inhalation • Used in major surgery. Examples: N2O, flurane gases, propofol LOCAL: • Block pain at site
where drug administered • Allows consciousness to be maintained • Administration route: topical,
intradermal, subcutaneous, epidural, intrathecal, intravenous. • Uses: dental surgery; suturing of
skin lacerations; minor surgery at a localised area; epidural Examples: lignocaine; amethocaine;
bupivicaine
- Pain • Pain is an
unpleasant sensory and
emotional experience
associated with actual or
potential tissue damage
(warning system!!!) • Pain
threshold varies from
individual to individual •
Pain tolerance involves
emotional aspects
- • Analgesia:
controlling
pain by
blocking pain
pathways
without loss
of sensation •
Anaesthesia:
prevention of
pain by
causing loss
of sensation
- • Analgesia:
controlling
pain by
blocking pain
pathways
without loss
of sensation •
Anaesthesia:
prevention of
pain by
causing loss
of sensation
- Narcotic: mimic natural peptides in our bodies (endorphins) • The effects of narcotic from therapeutic to overdose
includes analgesia, sedation, hypnosis, coma and finally death** benzos... • Morphine ‐ short half life (4 hrs) so dosing
has to be frequent; tolerance develops • Pethidine – used in child birth and surgery for mild to severe pain ‐ causes
less respiratory depression than morphine ‐ does not cause constipation. • Codeine • Fentanyl epidural (intrathecal)
transdermal patch (Duragesic®) lollipop (Actiq®) • Tramadol • Methadone ‐ used as a substitute for morphine and
heroin addiction as has lesser withdrawal symptoms ‐ 24 hrs half life ‐ strong analgesic NSAIDS AND COX2 -nausea,
vomiting, ulcerations, and headache AND gi. PARACETAMOL- metabolised in the liver and can cause hepatotoxicity
(alcoholics especially).
- Narcotic-opium (morphine/codeine/ pethidine/fentanyl) bind to opioid receptors stop subtance p .
liver high pass effect lwr dose result. kidney and bile out. Paracetamol, COX-2 inhibitors and NSAIDs
are PG synthesis inhibitors • Paracetamol – unknown what enzyme/s are inhibited • COX-2 inhibitors
– inhibits cyclooxgenase 2 enzyme (COX-2) • NSAIDs – inhibits cyclooxgenase enzymes (COX-1
BALANCING and COX-2 PROTECTIVE) GENRAL • nitrous oxide • isoflurane • desflurane •
sevoflurane • propofol • thiopentone (Pentothal) LOCAL• lignocaine (Xylocaine) • amethocaine • bupivacaine
• cocaine BLOCK PAIN
- control or relive pain
- aim to reduce with minmum effects 1. Affecting the
movement of sodium ions across the membrane
Examples: Phenytoin (Dilantin); Carbamazepine
(Tegretol) 2. Stabilising the nerve membranes directly
Examples: Ethosuximide 3. Affecting the activity of
Gamma‐amino butyric acid (GABA) Examples:
benzodiazepines (enhances the inhibitory action of
GABA); barbiturates (enhances the inhibitory action of
GABA); vigabatrin (inhibits the enzyme that degrades
GABA).CNS depressants Suppress abnormal electric
impulses from the seizure focus to other cortical areas.
- Drugs that have combined action: 1. Valproic acid (Valproate):
triggers release of GABA and inhibits sodium channels. 2.
Lamotrigine: inhibits passage of sodium through voltage sensitive
channels and reduces the release of glutamate (an excitatory
amino acid).
- • GI upsets • headaches • mental
confusion • nystagmus • allergic skin
rash • Myelosuppression and sedation
- Drug‐Drug Interactions • The majority of the
anticonvulsants are metabolised in the liver by the
microsomal P450 liver enzymes. Some exceptions are
gabapentin and vigabatrin. • Can affect their own
metabolism • May affect the metabolism of other
drugs as well.
- Drug‐Drug Interactions • The majority of the
anticonvulsants are metabolised in the liver by the
microsomal P450 liver enzymes. Some exceptions are
gabapentin and vigabatrin. • Can affect their own
metabolism • May affect the metabolism of other
drugs as well.
- • GI upsets • headaches • mental
confusion • nystagmus • allergic skin
rash • Myelosuppression and sedation
- Drugs that have combined action: 1. Valproic acid (Valproate):
triggers release of GABA and inhibits sodium channels. 2.
Lamotrigine: inhibits passage of sodium through voltage sensitive
channels and reduces the release of glutamate (an excitatory
amino acid).
- pain
- Used for people who cycle between mood swings
- Lithium carbonate (Lithicarb)::both manic and depressive state • Acts by enhancing the action of
amine reuptake pump and inhibit noradrenaline release,Narrow therapeutic index
drug‐....carbamazepine (BENZO) (Tegretol) and sodium valproate (Epilim) and lamotrigine
- LITHIUM treated like sodium,BLOODS ++ • Initially – slight nervousness, abdominal pain, anorexia,
vomiting, diarrhoea • Giddiness, tremor, ataxia, slurred speech, depression • Oliguria, hypovolaemia,
convulsive movements, coma • Potentially fatal outcome‐ cardiovascular, renal, failure •
Hypothyroidism, nephrogenic diabetes insipidus (polyuria, polydipsia)...
- LITHIUM treated like sodium,BLOODS ++ • Initially – slight nervousness, abdominal pain, anorexia,
vomiting, diarrhoea • Giddiness, tremor, ataxia, slurred speech, depression • Oliguria, hypovolaemia,
convulsive movements, coma • Potentially fatal outcome‐ cardiovascular, renal, failure •
Hypothyroidism, nephrogenic diabetes insipidus (polyuria, polydipsia)...
- Lithium carbonate (Lithicarb)::both manic and depressive state • Acts by enhancing the action of
amine reuptake pump and inhibit noradrenaline release,Narrow therapeutic index
drug‐....carbamazepine (BENZO) (Tegretol) and sodium valproate (Epilim) and lamotrigine
- antiepileptics
- Benzodiazepines • Most have a suffix “–azepam” • Potentiates the
inhibitory effect of gamma‐aminobutyric acid (GABA), a natural
inhibitory neurotransmitter • GABA increases influx of chloride
ions into the neuron which leads to hyperpolarisation and
decreased excitability
- • Anxiety and panic
disorders – anxiolytics •
Sleeping disorders –
hypnotics, sedative • Muscle
spasms and seizure
disorders – muscle
relaxants; anticonvulsants •
Preoperative medication
- • Majority lipid soluble and readily
absorbed from GIT • Widely
distributed in body and brain; highly
protein bound • Liver metabolism;
excretion via kidney • Half life ‐ helps
to determine which one to use
- • Adverse effects – commonly cause excess CNS depression • Drug Interactions – e.g. other CNS
depressants • Tolerance and dependence • Chronic administration – tolerance to sedation •
Dependence – can lead to overuse and abuse • Withdrawal symptoms ‐ CNS stimulation e.g. Anxiety,
sleep disorders, nervousness, seizures • Can cross placenta and into breast milk
- Other Anxiolytic/Sedative/Hypnotic Drugs • Barbiturates • Antihistamines • Buspirone • Zopiclone
and zolpidiem • Chloral hydrate
- Other Anxiolytic/Sedative/Hypnotic Drugs • Barbiturates • Antihistamines • Buspirone • Zopiclone
and zolpidiem • Chloral hydrate
- • Majority lipid soluble and readily
absorbed from GIT • Widely
distributed in body and brain; highly
protein bound • Liver metabolism;
excretion via kidney • Half life ‐ helps
to determine which one to use
- • Anxiety and panic
disorders – anxiolytics •
Sleeping disorders –
hypnotics, sedative • Muscle
spasms and seizure
disorders – muscle
relaxants; anticonvulsants •
Preoperative medication
- mood stabillisers
- Dopamine receptor–blocking activity in the brain: All of the
first generation and most of the second- generation
antipsychotic drugs block dopamine receptors in the brain
and the periphery (except clozapine-like atypical). – The
clinical efficacy of the typical antipsychotic drugs correlates
closely with their relative ability to block D2 receptors in the
mesolimbic system of the brain
- OLD.TYPICAL • Phenothiazines – chlorpromazine
Largactil (solution inj, tablet) – fluphenazine
Modecate (depot injection) – methotrimeprazine
(solution inj, tablet) • Thioxanthines –
zuclopenthixol (solution inj; tablet) – flupenthixol
Fluanxol (depot inj) • Butyrophenones – haloperidol
Serenace (tablet, liquid; inj) – pimozide Orap
(tablets) NEW-SECOND GEN-ATYPICAL Clozapine
(oral suspension, tablet) Olanzapine (wafer, tablet,
solution inj) Risperidone (oral solution, suspension,
tablet; long acting inj) Quetiapine (tablet)
- OLD::• Extrapyramidal effects ADOPT (Akathisia (restless) Dystonia
(spams) Oculogyric ( rolling eye) Parkinsonism (tremors) Tardive
(unreversiable ticks) ) • Postural hypotension • Anticholinergic •
Sedation • Weight gain • Endocrine effects ‐ e.g.
hyperprolactinaemia • Neuroleptic Malignant Syndrome (NMS)
ATYPICAL:: • Weight gain, dyslipidaemia‐ increased risk of CVD •
Diabetes type 2 ‐ especially with Clozapine and Olanzapine‐ due to
insulin antagonist effect – impair glucose entry into cells + impair
lipolysis in adipose tissue • Therefore –assess risk factors for
metabolic syndrome etc, family history, monitor‐ blood tests •
Agranulocytosis – Clozapine; therapeutic monitoring BOTH;;;
- note: can
effect
people
hours
days
years
- note: can
effect
people
hours
days
years
- OLD::• Extrapyramidal effects ADOPT (Akathisia (restless) Dystonia
(spams) Oculogyric ( rolling eye) Parkinsonism (tremors) Tardive
(unreversiable ticks) ) • Postural hypotension • Anticholinergic •
Sedation • Weight gain • Endocrine effects ‐ e.g.
hyperprolactinaemia • Neuroleptic Malignant Syndrome (NMS)
ATYPICAL:: • Weight gain, dyslipidaemia‐ increased risk of CVD •
Diabetes type 2 ‐ especially with Clozapine and Olanzapine‐ due to
insulin antagonist effect – impair glucose entry into cells + impair
lipolysis in adipose tissue • Therefore –assess risk factors for
metabolic syndrome etc, family history, monitor‐ blood tests •
Agranulocytosis – Clozapine; therapeutic monitoring BOTH;;;
- OLD.TYPICAL • Phenothiazines – chlorpromazine
Largactil (solution inj, tablet) – fluphenazine
Modecate (depot injection) – methotrimeprazine
(solution inj, tablet) • Thioxanthines –
zuclopenthixol (solution inj; tablet) – flupenthixol
Fluanxol (depot inj) • Butyrophenones – haloperidol
Serenace (tablet, liquid; inj) – pimozide Orap
(tablets) NEW-SECOND GEN-ATYPICAL Clozapine
(oral suspension, tablet) Olanzapine (wafer, tablet,
solution inj) Risperidone (oral solution, suspension,
tablet; long acting inj) Quetiapine (tablet)
- anxiolytics
- overall mode of action is to… increase levels and activity
of the excitatory neurotransmitters ‐ serotonin,
noradrenaline...• First choice antidepressants ‐ SSRIs,
RIMA, reboxetine, venlafaxine
- • Major groups: SSRIs; MOAIs; TCAs; RIMAs •
Tetracyclic antidepressants ‐ maprotiline, mianserin
Block the presynaptic (α2) receptors and
noradrenaline re‐uptake and possibly serotonin
action • Noradrenaline re‐uptake inhibitors (NRIs)‐
Reboxetine • Serotonin and noradrenaline reuptake
inhibitor (SNRI) – venlafaxine • St John’s wort ‐
‘Natural remedies’ OTCs
- ONSET: TAKE TIME ADVERSE +++++
- ADVERSE; AND DRUG INTERACTIONS
- TCAs anticholinergic; antiadrenergic (postural
hypotension) antihistaminic (sedative); weight gain;
cardiac arrhythmias MAOIs anticholinergic;
adrenergic; risk of hypertensive crisis; sedation
RIMAs lower risk of adrenergic; nausea; insomnia;
headache SSRIs nausea; insomnia; sexual
dysfunction
- TCAs other antidepressants; antimuscarinics; hypnotics;
anxiolytics; anesthetics; antihypertensives; caution with
antiepileptics MAOIs sympathomimetics(e.g. L‐DOPA,
isoprenaline; pseudoephedrine etc); other antidepressants;
antihistamines; hypnotics; anxiolytics SSRIs other
antidepressants; antiepileptics; antipschotics; other drugs
that increase serotonin (e.g St Johns Wort; tramadol etc)
- TCAs other antidepressants; antimuscarinics; hypnotics;
anxiolytics; anesthetics; antihypertensives; caution with
antiepileptics MAOIs sympathomimetics(e.g. L‐DOPA,
isoprenaline; pseudoephedrine etc); other antidepressants;
antihistamines; hypnotics; anxiolytics SSRIs other
antidepressants; antiepileptics; antipschotics; other drugs
that increase serotonin (e.g St Johns Wort; tramadol etc)
- TCAs anticholinergic; antiadrenergic (postural
hypotension) antihistaminic (sedative); weight gain;
cardiac arrhythmias MAOIs anticholinergic;
adrenergic; risk of hypertensive crisis; sedation
RIMAs lower risk of adrenergic; nausea; insomnia;
headache SSRIs nausea; insomnia; sexual
dysfunction
- ONSET: TAKE TIME ADVERSE +++++
- MODE OF ACTION
- • Major groups: SSRIs; MOAIs; TCAs; RIMAs •
Tetracyclic antidepressants ‐ maprotiline, mianserin
Block the presynaptic (α2) receptors and
noradrenaline re‐uptake and possibly serotonin
action • Noradrenaline re‐uptake inhibitors (NRIs)‐
Reboxetine • Serotonin and noradrenaline reuptake
inhibitor (SNRI) – venlafaxine • St John’s wort ‐
‘Natural remedies’ OTCs
- Definition • A sedative is a substance that diminishes the activity of an organ or tissue, in our
context‐ CNS • Hypnotic (sleeping pills) is a substance that induces sleep • Anxiolytics (minor
tranquilisers) are substances that alleviate anxiety
- antipsychotics
Media attachments
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Want to create your own Mind Maps for free with GoConqr? Learn more.