6468356
Description
Flashcards by Andrew Street, updated more than 1 year ago
|
|
Created by Andrew Street
over 8 years ago
|
|
| Question | Answer |
| 941 Define HT. | Grade 1 (mild) = 140-159 &/or 90-99 (diastolic) Grade 2 (moderate) = 160-179 &/or 100-109 Grade 3 (severe) = >180/>110. K & C p777. |
| 941 Give British Hypertension Society targets for BP control. | Optimal treated BP pressure: <140/85 (no DM) or <130/80 (with DM). |
| 944 What factors are associated with essential HT? | Essential HT (80-90% of cases of HT) - whilst it is of unknown cause it is multifactorial involving: genetic factors / fetal factors (low birth weight is associated with ^BP) / environmental factors (obesity, alcohol, Na+ intake, stress). K & C p777. |
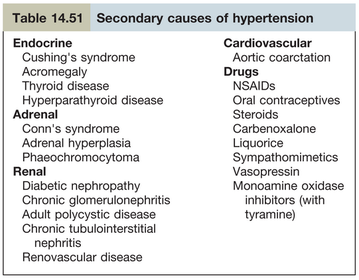
| 944 List secondary causes of HT. | |
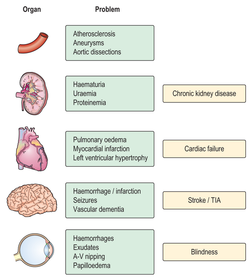
| 944 Describe the end organ damage caused by HT. | |
| 945 Describe S & Sx of HT. | The pt with mild HT is usually asymptomatic. Attacks of sweating, headaches & palpitations point towards the diagnosis of phaeochromocytoma. Higher levels of BP may be associated with headaches, epistaxis or nocturia. Breathlessness may be present owing to left ventricular hypertrophy or cardiac failure, while angina or Sx of peripheral arterial vascular disease suggest the diagnosis of atheromatous renal artery stenosis. This is usually a local manifestation of more generalized atherosclerosis, and patients are often elderly with co-existent vascular disease. Fibromuscular disease of the renal arteries encompasses a group of conditions in which fibrous or muscular proliferation results in morphologically simple or complex stenoses and tends to occur in younger patients. Malignan HT may present with severe headaches, visual disturbances, fits, transient loss of consciousness or symptoms of heart failure. k & C p779. |
| 947 List associated cardiovascular risk factors that should be looked for in pt's with HT. | According to the NICE HT Guidelines: For all people with HT offer to: * test for the presence of protein in the urine by sending a urine sample for estimation of the albumin:creatinine ratio and test for haematuria using a reagent strip * take a blood sample to measure plasma glucose, electrolytes, creatinine, eGFR, serum total cholesterol and HDL cholesterol * examine the fundi for the presence of hypertensive retinopathy * arrange for a 12-lead electrocardiograph to be performed. |
| 948 As part of an examination of a pt with HT what clinical signs should be sought that may reveal an underlying cause or subsequent effects? | * Renal artery bruits - renovascular HT * Radiofemoral delay - coarctation of the aorta * Cardiac examination may reveal signs of LVH & a loud 2nd HT sound * If cardiac failure develops there may be a sinus tachycardia & a 3rd HT sound * Fundoscopy - tortuosity of the retinal arteries, arteriovenous nipping, haemmorhages, soft exudates, papilloedema. K & C. |
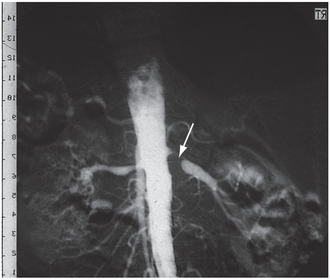
| 944 What potential cause of HT does this angiograph show? | Digital subtraction angiography, showing typical unilateral atheromatous renal artery stenosis with post-stenotic dilatation (arrow). K & C. |
| 944 What hypertensive changes are seen in this fundus? | Fundus showing hypertensive changes: Grade 4 retinopathy with papilloedema, haemorrhages and exudates. K & C. |
| 950 List the non-pharmacological Rx that should be recommended to a pt with HT. | BMJ Best Practice: * Sodium reduction (≤2.4 g/day) * Dietary approaches - 8-10 servings of fruit and vegetables daily, whole grains, low sodium, low-fat proteins * Maintaining waist circumference of <102 cm for men and <88 cm for women * Weight loss to a BMI of about 25 kg/m^2 * ^Physical activity consisting of at least 30 minutes of moderate intensity, dynamic aerobic exercise (walking, jogging, cycling, or swimming) 5 days per week to total 150 minutes/week, as tolerated or recommended by physician; * Limited alcohol consumption (<2-3 standard drinks/day in hypertensive men; <1-2 standard drinks/day in hypertensive women). Total weekly consumption <14 standard drinks (140 g) for men and 8 standard drinks (80 g) for women. |
| 951 Outline the NICE Guidelines Treatment Steps for HT. https://pathways.nice.org.uk/pathways/hypertension/treatment-steps-for-hypertension | |
| 952 Define accelerated/malignant HT & describe the pathology of target organ damage caused by accelerated HT. | Hypertensive emergencies include both accelerated HT & malignant HT. In both cases a recent ^BP to very high levels (≥180 mm Hg systolic & ≥110 mm Hg diastolic) results in target organ damage - usually seen as neurological (eg encephalopathy), cardiovascular or renal damage. The term malignant HT is usually reserved for cases where papilloedema is present. http://patient.info/doctor/hypertensive-emergencies |
| 953 Mx of malignant/accelerated HT. | General measures The aim is to reduce the blood pressure over 24-48/24. Pt's usually have altered BP autoregulation & if the BP is reduced too fast, there may be organ hypoperfusion. Initially, try to reduce the mean arterial pressure by approximately 25% over the first 24-48/24. An arterial line is helpful for continuous BP monitoring. There may be severe sodium & volume depletion; volume expansion with isotonic sodium chloride solution may be required. Drugs Initially, an IV route is usually used. Nitroprusside is often used as an IV drug but labetolol or nicardipine are alternatives which can be switched to oral formulations once blood pressure control is achieved. There is, however, some evidence that labetalol may produce a greater reduction in peripheral BP in the immediate Rx of malignant HT. http://patient.info/doctor/hypertensive-emergencies |
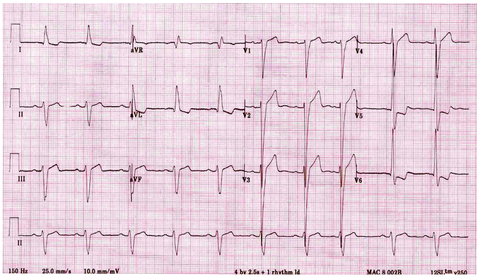
| What ECG change is seen here that may be due to HT & what criteria may be used to Dx it? | LVH. The most commonly used criteria for diagnosing LVH is the Sokolov-Lyon criteria (S wave depth in V1 + tallest R wave height in V5-V6 > 35 mm). http://lifeinthefastlane.com/ecg-library/basics/left-ventricular-hypertrophy/ |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Want to create your own Flashcards for free with GoConqr? Learn more.