795018
Description
Flashcards by sophietevans, updated more than 1 year ago
|
|
Created by sophietevans
over 10 years ago
|
|
| Question | Answer |
| When does extrinsic control (i.e. extrinsic to an organ; hormones, neural control) become necessary over intrinsic control? | When homeostasis is tested (e.g. exercise) and there is competition for blood flow between organs. |
| What effects does the autonomic nervous system anticipatory response have on the body? | The anticipatory response begins before activity even starts (hence the name) and increases heart rate, stroke volume, and therefore blood pressure. |
| In a challenge to homeostasis such as exercise, the autonomic nervous system regulates bodily functions. Sympathetic activity is increased, while parasympathetic activity is decreased. List some effects of increased sympathetic activity. | Increased blood pressure, increased heart rate (via SA node), increased stroke volume, increased venomotor tone (leading to increased stroke volume as more blood is returned to the heart), increased cardiac output as a result of increased HR and SV, and increased blood glucose through effect on the pancreas. |
| Muscles (predominately skeletal muscles) convert what percentage of ATP into external work? Where does the remaining percentage go? | ~20% of ATP is used for external work, whereas the remaining ~80% is converted into heat (therefore it is very important that the body is able to lose heat). |
| Do long-term (e.g. oxidative phosphorylation), intermediate, and short-term energy systems operate separately? | No, they operate together, and none are finite. |
| List four initial energy sources from muscle stores available for substrate level phosphorylation. | ATP, creatinine, glucose, and glycogen. |
| Why is the energy for prolonged activity dependent on blood flow? | Because blood delivers oxygen, glucose, and fatty acids, all of which are required for activity, and removes the products of activity (CO2, heat, lactic acid, any Ca2+ passing across the sarcolemma). |
| What is lactate converted into when O2 is present? | Pyruvate. |
| Metabolic demands of active muscles must be met without compromising the energy supply to which two organs? | Brain + heart. |
| The mobilisation of energy stores for activity is primarily under hormonal control - which is the major hormone involved? | Glucagon is the 'post-absorptive state' hormone which is increased in increased activity to release energy stores. Alternatively, insulin is the 'absorptive state' hormone, which is decreased during increased activity so that release of substrates is promoted. |
| Other than glucagon, name two less important regulators of the mobilisation of energy stores in exercise. | Epinephrine and sympathetic nervous stimulation. |
| List some of the actions of insulin when it is released from the beta cells of the pancreatic islets of Langerhans. | In most tissues there is an increase in the uptake of glucose (except the brain, liver, and exercising muscle), as well as amino acid uptake and an increase in protein synthesis, and a decrease in protein catabolism. In adipose tissue there is an increase in fatty acid and triglyceride synthesis, and a decrease in lipolysis. In liver and muscle tissue there is an increase in glycogen synthesis and a decrease in glycogenolysis. In the liver there is an increase in fatty acid and triglyceride synthesis and a decrease in gluconeogenesis. Overall, insulin is an 'absorptive state' hormone and so its effects are generally anabolic. |
| List some of the effects of glucagon when it is released from the alpha cells of the pancreatic islets of Langerhans (in response to decreased plasma glucose, epinephrine secretion, increased plasma amino acids, and increased sympathetic activity). | In the liver, there is increased glycogenolysis and gluconeogenesis, as well as increased ketone synthesis and protein catabolism, and decreased glycogen and protein synthesis. In the adipose tissue, there is increased lipolysis and decreased triglyceride synthesis. Overall, glucagon is a 'post-absorptive state' hormone, which has catabolic effects to provide nutrients. |
| How does plasma glucose concentration affect the sympathetic nervous system? | Decreased plasma glucose is detected by glucose receptors in the central nervous system. This increases sympathetic activity leading to all of its effects, including increasing glycogenolysis and gluconeogenesis in the liver and lipolysis in the adipose tissue, and stimulating the adrenal medulla to secrete epinephrine which acts on muscle to increase glycogenolysis. These result in increased plasma glucose concentration, which results in negative feedback which reduces epinephrine secretion. |
| How does sex (male/female) influence the use of energy sources? | In males, higher blood epinephrine stimulates glycogenolysis in liver and muscle, so more carbohydrates are liberated as an energy source. In females, oestrogens increase lipolysis in muscle and adipose tissue, and inhibit gluconeogenesis and glycogenolysis, resulting in the liberation of fats as an energy source. |
| Give an examine of a local factor to blood vessels, the release of which results in vasodilation. | Nitric oxide - its release opens up capillary beds in muscles, allowing for better perfusion and delivery of O2/removal of CO2. |
| Up to 20x more blood flow to a muscle can be delivered during activity. What proportion of capillaries in a skeletal muscle vascular bed is open at rest? | Only one in every 30-40 capillaries. |
| List 5 factors which result in vasodilation. | Decreased pO2 and increased pCO2, decreased pH (as a result of increased pCO2), increased extracellular [K+], and increased temperature. All but temperature are local factors which can act on small arterioles and precapillary sphincters to dilate smooth muscle. The changes are also detected by chemoreceptors, specialised free nerve endings that send the information to the CNS, which will then increase ventilation and cardiac output. Temperature, on the other hand, is detected by thermoreceptors, which relay information to the hypothalamus, resulting in a systemic response. |
| At rest cardiac output is ~5L/min. What are the specific values for CO for males and females? | Males: ~5.6L/min. Females: ~4.9L/min. |
| Under resting conditions, blood flows through pulmonary capillaries in around 1 second and gas exchange is completed by ~1/3 of the capillary. How does this differ during activity? | The cardiac output is increased from ~5 L/min to >15 L/min. The pulmonary pressure increases, and blood flows faster through the lungs. The remaining 2/3 of capillary length is utilised for gas exchange up to a cardiac output of ~30 L/min. |
| In elite athletes, at high cardiac outputs, desaturation of haemoglobin can occur. Why? | Potentially because increased stroke volume increases the pressure through the lungs such that gas exchange is decreased. |
| During exercise, there is increased blood flow to the heart in order for it to work at a higher intensity than at rest. Is this under local or systemic control? | Generally it is under local control. However, circulating adrenaline may contribute to the activation of beta2-receptors to have both a chronotropic and an inotropic affect. |
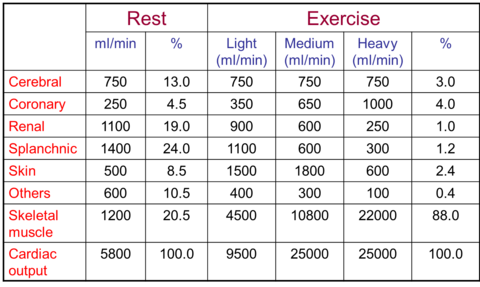
| Here is a table of the changes in volumes of blood delivered to different tissues in exercise compared to rest. In marathon runners, the large decrease of 1100 ml/min in light exercise to 300 ml/min in heavy exercise in the splanchnic blood supply is no biggie - but in ultra endurance runners, this can result in the development of ischaemia and tissue damage in the guy as a result of this activity long term. | |
| Vasodilation leads to an increase in the number of capillaries carrying blood through muscles. What does this mean for O2 and mitochondria? | More capillaries carrying blood through muscles means there is a decreased distance between capillaries and mitochondria in muscle fibres, and therefore an increase in O2 offloading from haemaglobin. This offloading is assisted by an increase of pCO2, temperature and acidity in the muscle tissue. |
| In a haemaglobin-oxygen dissociation curve (in which pO2 is plotted on the x axis and %O2 saturation of haemaglobin is plotted on the y axis), what effect would increasing pCO2/decreasing pH have? | The curve relating pO2 to %Hb(sat) would shift right as haemaglobin had decreased affinity for oxygen due to increased pCO2/decreased pH, meaning that the partial pressure of oxygen would need to be increased to meet the same level of saturation. |
| What is Starling's law? | The heart will pump whatever is returned to it - so if the end diastolic volume is increased and the end systolic volume is decreased, even though diastolic filling time is decreased due to an increased heart rate, the stroke volume must be increasing to shift the increase in blood returned to it. |
| Why is the baroreceptor reflex for controlling blood pressure not active during exercise? | Because of the compression of blood vessels by contracting skeletal muscles - if blood pressure is REQUIRED to be increased, as by exercise, there is no point in the body trying to decrease it. This is the case when increased sympathetic activity in exercise prevents the baroreceptors from acting. |
| What is the primary mechanism for controlling the mean arterial blood pressure in exercise? | Regulation by central command to the cardiovascular control centre. Metaboreceptors in the muscles only contribute to cardiovascular control at high intensity exercise. |
| Why does pulse pressure increase in exercise? | Because systolic pressure increases and diastolic pressure decreases (as a result of vasodilation). |
| Why is it good to have a lower resting heart rate? | Because this leaves a larger range for possible increase in exercise, and for gauging the appropriate increase. |
| If Mean Arterial Blood Pressure = Cardiac Output x Total Peripheral Resistance, an increase in cardiac output leads to an increase in mean arterial blood pressure when...? | When total peripheral resistance remains the same or increases. |
| If Mean Arterial Blood Pressure = Cardiac Output x Total Peripheral Resistance, a constant cardiac output leads to an increase in mean arterial blood pressure when...? | When total peripheral resistance increases. |
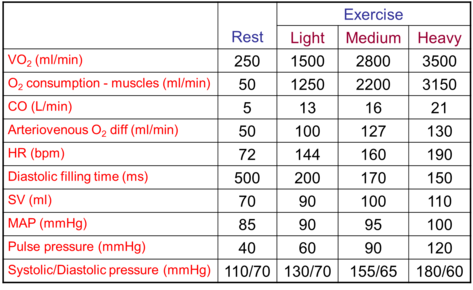
| Here's a table of some cardiovascular changes during exercise. Systolic blood pressure tends to increase more significantly than diastolic pressure (given that less diastolic pressure is needed and vasodilation limits it anyway). There is a bigger difference between arterial O2 and venous O2 the higher the exercise intensity. | |
| Increased gas exchange is required in exercise. How does one increase ventilation? | Increasing tidal volume (tends to be in low to moderate exercise intensities) and frequency (tends to be in higher exercise intensities). |
| In order to increase ventilation (either by increasing tidal volume or frequency), what changes are required? | Increased activity of respiratory muscles (these take around 15% of the cardiac output during exercise, and need a fairly significant amount of O2/nutrients to generate ATP for their contraction), and decreased work to breathe. The latter is achieved by the presence of adrenaline (released by sympathetic stimulation of the adrenal medulla) which causes bronchodilation, releasing bronchus resistance to air flow. There is also orderly recruitment of the respiratory muscles in order to maximise their efficiency, and coordinated skeletal muscle activity e.g. coordinating arm/leg activity and/or breathing which increases efficiency (learned activity). |
| You cannot train your lungs in order to increase efficiency during exercise. What can you train to affect ventilation? | Inspiratory muscles and/or coordination of skeletal muscle contract (e.g. when running) with breathing. |
| In submaximal exercise, arterial O2 and CO2 concentrations are kept relatively constant. How? | Increased tidal volume and frequency as a result of neuronal input to the respiratory centre from the motor cortex (and a small amount due to detection of increased pCO2 and decreased pH by chemoreceptors) is sufficient to increase exercise-ventilation with exercise intensity. |
| All pulmonary capillaries are recruited for gas exchange when cardiac output exceeds how many times the resting value? | 3x |
| During maximal exercise, how does hyperventilation result? | There is a disproportionate increase in minute volume and VCO2 during high intensity exercise, as a result of additional stimulation of carotid bodies, the onset of lactate accumulation in the blood, and the appearance of other stimuli e.g. K+ ions. |
| What is the ventilatory threshold? | The point at which sufficient chemoreceptors have been activated to increase the ventilatory rate. |
| What is an incremental activity exercise? | An exercise in which O2 consumption during activity is gradually increased in a stepwise manner in order to measure it. |
| In sprint/power events, the relationship between physiological measures and the performance is poor. However, in endurance athletes performance correlates well with two physiological measures. What are these? | Lactate threshold and VO2-max. Both of these give a good measure of endurance performance, rather than power, for instance. These are normally assessed using an incremental exercise test. |
| At the highest levels of exercise intensity, O2 consumption begins to reach a... | ...plateau. |
| VO2-max relates to both the O2 supply (maximum cardiac output) and O2 use by the muscles (arteriovenous O2 difference). What is the equation to show this relationship? | VO2-max = max cardiac output x arteriovenous O2 difference. Training can increase VO2 max, but this is ~50% dependent on genetic determinants of VO2 max (as 50% of VO2-max differences are genetically determined). Elite endurance athletes have a high VO2 max. |
| In which units is VO2 max usually expressed? | L/min or ml/kg/min. |
{kind=link}
{kind=link}
Want to create your own Flashcards for free with GoConqr? Learn more.