6794660
Description
Mind Map by Farah Mansour, updated more than 1 year ago
|
|
Created by Farah Mansour
about 8 years ago
|
|
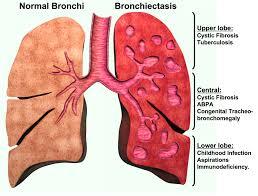
Bronchiectasis
- Permanent DILATION of the bronchi and bronchioles
causing repeated episodes of airway infection and
inflammation << Due to destruction of cartilage and
elastic tissue by chronic necrotizing infections
- Causes
- Cystic fibrosis
- Autosomal recessive disease
- Pathogenesis
- (1) Most common mutation is a three-nucleotide
deletion on chromosome 7 that normally codes
for phenylalanine (70% of cases).
- (2) Mutation causes defective protein folding in the
cystic fibrosis transmembrane conductance
regulator (CFTR).
- (3) Defective CFTR is degraded in the Golgi apparatus.
- (4) Loss of CFTR causes decreased Cl– reabsorption in
the sweat glands
- Effect of loss of CFTR in
other secretions:
- (a) Increased Na+ and water reabsorption from
luminal secretions
- (b) Decreased Cl– secretion out of epithelial cells
into luminal secretions
- (c) Net effect of these electrolyte alterations is
dehydration of body secretions due to lack of NaCl.
- (a) Increased Na+ and water reabsorption from
luminal secretions
- (1) Most common mutation is a three-nucleotide
deletion on chromosome 7 that normally codes
for phenylalanine (70% of cases).
- Autosomal recessive disease
- Infections
- (a) TB is the most common cause worldwide.
- (b) Mycobacterium avium-intracellulare (typically involves the
right middle lobe and lingula), adenovirus, Staphylococcus
aureus, Haemophilus influenzae
- (a) TB is the most common cause worldwide.
- Bronchial Obstruction
- Primary ciliary dyskinesia
- (a) Dynein arm in cilia is absent.
- (b) Dynein arm contains ATPase (adenosine
triphosphatase) for movement of the cilia.
- (a) Dynein arm in cilia is absent.
- Allergic bronchopulmonary aspergillosis
- Cystic fibrosis
- Gross Findings
- a. Most commonly occurs in the lower lobes
- b. Dilated bronchi and bronchioles are filled
with pus
- (1) Dilated airways extend to the lung
periphery.
- (2) Dilations are tube-like
and/or saccular.
- (1) Dilated airways extend to the lung
periphery.
- a. Most commonly occurs in the lower lobes
- Clinical
Findings
- a. Cough productive of copious sputum (often cupfuls)
- b. Hemoptysis that is sometimes massive
- c. Digital clubbing
- d. Cor pulmonale
- Chest cardiograph & CT scan Findings
- Crowded bronchial markings extend to the lung periphery
- Crowded bronchial markings extend to the lung periphery
- a. Cough productive of copious sputum (often cupfuls)
Media attachments
{kind=link}
Want to create your own Mind Maps for free with GoConqr? Learn more.