544666
Description
Mind Map by katpotter71, updated more than 1 year ago
|
|
Created by katpotter71
almost 11 years ago
|
|
Nervous
System
- Central Nervous System (CNS)
- Peripheral Nervous System (PNS)
- Somatic Nervous System
Annotations:
- Drives the skeletal muscles => sometimes referred to as the voluntary NS
- Add link to ACh nicotinic
- Autonomic Nervous System
Annotations:
- Sympathetic and parasympathetic NS control all the things you do without thinking => they function by receiving information from the periphery, sending info to the brain, the brain processing and sending back a signal to change if necessary => a reflex loop
- All the autonomic NS has the same sort of structure => there is a nerve coming from the spinal cord, then a ganglion and then another nerve => second nerve interacts with target organ a ganglion is a synapse between two nerves => it is too small to be seen under a microscope => looks like a swelling in the nerve => it releases neurotransmitters from the preganglionic nerve onto the postganglionic nerve There is also a synapse between the post-ganglionic nerve and the target organ => this synapse is sometimes referred to as the neuroeffector junction => the nerve is affecting a non-neuron cell
- Parasympathetic NS
Annotations:
- Parasympathetic nerves tend to leave right at the base of the neck (cranial outflow) or at the base of the spinal cord (sacral outflow) => go out towards various organs (eyes, airways, salivary glands, heart, GI tract, bladder, reproductive organs & large intestine) => preganglionic nerves are long and post-ganglionic are short
- The neurotransmitter in the parasympathetic NS is the same for all synapses: acetylcholine => however, have two different types of receptors: => in the ganglia, have Nicotinic acetylcholine receptors => in the neuroeffector junction, have muscarinic receptors These two types of receptors are different in their structures, operation and pharmacology => this is good, as we can give drugs that differentiate between them => e.g. can give a drug that targets a muscarinic receptor in the gut and it won't touch the nicotinic receptors => good for reducing side effects
- Parasympathetic does generally the opposite to the sympathetic => slows down heart rate (doesn't generally affect force => keeps heart beat slow (natural heart beat without input from parasympathetic ns is about 90 beats/min) => salivary glands => secrete thin, watery secretions => contain lots of enzymes => tend to digest while resting => airways constrict => less O2 => pupils contract => focuses eyes for near vision => GI tract => increases peristalsis and secretions => digest when at rest
- Activity
modification
via drugs
Annotations:
- Need to know which drugs you can put in these pigeon holes
- Pre-synaptically
- Synthesis
Annotations:
- Don't have any clinically useful drugs that act here
- To block the synthesis of ACh => can block the transporter protein that transports in the choline precursor which is critical for ACh production => hemicholiniums can block this transporter => not used clinically but have been used as insectisides => also a problem with them is that they take a very long time to take effect => already have lots of ACh stored in nerve terminal => have to wait for stores to be depleted before seeing any effect=> there is no known way to block the CAT enzyme which is the key enzyme involved in the synthesis of ACh
- Storage
Annotations:
- Don't have any clinically useful drugs that act here
- Can inhibit the transporter molecule that packages ACh => Vesamicol => not used clinically because again, already have lots of stores of ACh built up => takes several hours to see any effect => very slow in producing any effect
- Release
Annotations:
- Can block the calcium channels => by using another cation e.g. magnesium => is larger than the calcium ion => tries to go through but gets stuck => however, lacks selectivity => calcium channels are found in every nerve terminal => so will block all neurotransmitters => not a clinically relevant target
- Botulinium toxin and Beta-bungarotoxin (a snake venom) interfere with the process of exocytosis => there is some degree of selectivity here towards cholinergic nerves => botulinium toxin gets transported into cholinergic nerves => not known why selective
- 'Bo-tox'
Annotations:
- Botulinium toxin - from Clostridium botulinum - is found in uncooked foods => ingestion of it gives rise to food poisoning => botulism Extremely potent toxin => lethal dose in mice is about 10tothe-12 grams => death occurs due to paralysis of respiratory muscles
- Has been used in chemical warfare => more recently used clinically (cosmetically) => used to treat wrinkles => NEVER given systemically => always small, local injections to desired muscle => permanent at molecular level => destroys key proteins involved in exocytosis (SNAP-25, Synaptobrevin & Syntaxin) => however nerves start to sprout new nerve endings after about 3 months
- Another clinical use is in the treatment of inappropriate muscle contraction => e.g. blepharospasm => eyelids contract and close => can't open eyes => also used to treat tension headaches => headache caused by tension in the muscles in the neck => some beneficial effect => also been used to treat some of the paralysis associated with cerebral palsy => used to treat hyperhidrosis (excess, inappropriate sweating => sweating is controlled by sympathetic ns but is the only part of sns that has ACh acting on a muscarinic receptor) => can inject botox locally (e.g. palms) to stop the inappropriate sweating => however, is painful to have lots of little injections into hand => now combine it with local anaesthetic Also trialing use in bladder hyperreactivity and spasticity associated with MS
- Link to MAChR
- Synthesis
- Post-synaptically
- Receptors
- NAChR
- Depolarising
Muscle Relaxants
Annotations:
- Only one clinically relevant drug that is an agonist of the NAChR, also known as a depolarizing muscle relaxant => Suxamethonium (also called succinylcholine)
- As an agonist, it has both affinity and efficacy => binds to the receptor and activates it => associated channel opens and produces a depolarization of the muscle membrane => unlike ACh, suxamethonium is not broken down by AChE => thus when suxamethonium is released into the synaptic cleft, it can bind to the receptor and come off, then go back on as it doesn't get broken down => causes a prolonged depolarization of the neuromuscular junction by repeated activation of the receptor
- To understand why this causes a neuromuscular block, we must understand how the voltage dependant sodium channels operate When the membrane depolarizes, the sodium channels open up, conduct sodium and then very quickly close down again => they are then in the inactivated state Once they are in the inactive state, they can't reopen again => they have to return to the resting state first => this happens very slowly => only when the membrane potential is back at it's resting value => this is called the refractory period
- Under normal physiological conditions, the action of ACh is very quick => because ACh is broken down very quickly by AChE => gives the membrane time to cycle back through the refractory period However, because Suxamethonium is not broken down by AChE => get a prolonged activation and a long lasting depolarization => so you get a first action potential but channels never get a chance to recover => being held in continuous depolarization due to the continued activation of the receptors
- The main clinical use is for rapidly reacting, short-duration muscle relaxation => main two are endotracheal intubation => can't stick a tube down the throat normally because of automatic gag reflex that protects the airways => so would want something that acts fast (as pt's that need a tube down their throat don't have time to wait for a slower muscle relaxant) => also used during Electroconvulsive Therapy (ECT) => to stop contractions caused by electrical currents However, pt's do complain of post-op muscle pain => this happens because the muscles (e.g. in arm) that usually work in opposition (e.g. one set flexes arm, one set straightens arm) are being forced to contract at the same time => in effect pulling against each other => causes pain for the pt
- Although it is not broken down by AChE it is broken down by Butarylcholine Esterase (BChE) => is found in the plasma (thus also known as plasma cholinesterase) Suxamethonium lasts in the body for about 10 min after being injected => the exception to this is in pt's that have a genetic deficiency in the BChE enzyme => for them it will last several hours => do NOT give anticholinesterase drugs (e.g. neostigmine) => will make symptoms worse => will have suxamethonium that isn't being broken down AND ACh that isn't being broken down
- Non-Depolarising
Muscle Relaxants
Annotations:
- Reversible competitive antagonists of the nicotinic acetylcholine receptor are often referred to as non-depolarizing muscle relaxants => they have affinity to the receptor but no efficacy => so they bind to the receptor but don't activate it => means that ACh can't bind to it either, so the receptor can't be activated => transmission doesn't occur Historicaly tubocurarine was used in poison darts=> able to use that to hunt because it is not orally active => has to be given by injection => not clinically useful anymore => modern day equivalents are vecuronium, atracurium, pancuronium
- Now used clinically as a muscle relaxant during surgery to allow lower doses of general anaesthesia => a sudden muscle spasm is unwanted during delicate surgery => have to prevent reflex muscle contraction It is possible to do this with general anaesthesia => lose pain when the brain is depressed about halfway (midbrain) => have to have a profound, deep depression of the brain activity to supress these reflexes => is possible but patient will be very close to death at that point => very close to being braindead => get around this by using muscle relaxant alongside the general anaesthetic => patient must be ventilated => skeletal muscles will be paralyzed as well => they are necessary part of breathing => can potentially be a problem if ga wears off during surgery => pt will be awake but unable to move and alert the team to the situation NOTE, this is not an anaesthetic, only a muscle relaxant => is not having any effect on the brain Effects last 15-40 min, depending on the drug
- Ganglion stimulants
Annotations:
- Nicotinic receptor agonist that preferentially act in the nicotinic receptors in the autonomic ganglia => e.g. nicotine, lobeline, DMPP => have no clinical use for these
- Nicotine
Annotations:
- Nicotine causes drug dependence by it's action in the CNS => not on the periphery The effects are: increased alertness, arousal, enhanced learning and reduced anxiety and tension It does have peripheral side effects => increased heart rate (tachycardia), increased cardiac output & BP, reduced GI mobility, sweating and nausea & vomiting (first time smokers) => over time pt develops tolerance to these side effects
- The harmful effects of smoking don't come from the nicotine but from other excipients in the smoke => e.g. cancer, coronary heart disease, emphysema => but nicotine is what causes the addiction
- Ganglion Blockers
Annotations:
- Ganglionic nicotinic receptor antagonists => also known as ganglion blockers => e.g. Hexamethonium trimetaphan Major effect is reduction of blood pressure => can cause postural hypotension => has very
- These drugs are not used very much anymore because of their widespread side effects => Trimetaphan sometimes used during surgery => because it causes BP to drop significantly => due to blocking the sympathetic ns => which is what maintains BP at a higher level => this is useful during surgery to reduce bleeding => a heart/lung machine is used to maintain the circulation => would never use this to treat high BP => i.e. would never send a pt home with a prescription for it
- Depolarising
Muscle Relaxants
- MAChR
- Parasympathomimetics
Annotations:
- Muscarinic receptor agonists => also known as parasympathomimetics => can easily develop drugs that are selective for muscarinic receptors => differentiate between nicotinic and muscarinicc easily => however not very good at developing drugs that differentiate between the different muscarinic receptor subtypes (M1, M2 & M3) => means that there is a potential for side effects => have limited clinical use because of this lack of selectivity Examples: pilocarpine, bethanacol
- Bethanacol
Annotations:
- used as a stimulant laxative and to treat urinary retention => has effects on the parasympathetic ns => on the gut and the bladder => stimulates peristalsis and increases muscle tension in the bladder (causes you to urinate)
- Sometimes after surgery, it can be difficult to get the organs going again => pt's can suffer from urinary retention or quite severe constipation => can give these short term (e.g. a few days) => gets the gut to start moving => to overcome the constipation => or to overcome the urinary retention
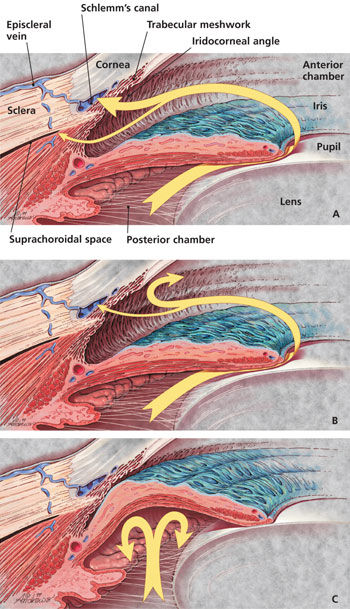
- Pilocarpine
Annotations:
- Quite commonly used to treat glaucoma
- Glaucoma is an increase in the intraocular pressure => i.e. pressure in the front of the eye Aqueous humour is a gelatinous, transparent fluid that fills the space between the lens and the cornea=> it is a filtrate of plasma => has to be filtered as plasma is a rather yellow, cloudy colour => wouldn't be able to see if it was that colour the ciliary body acts as a filter => filtering out proteins from the blood plasma => maintains the fluid => fluid drains away through canal of Schlemm => however, if fluid doesn't drain away => eye gets bigger and bigger => this usually happens due to a blockage of the drainage channels => this is called glaucoma => generally age-related => to confirm glaucoma => do an eye-test => see how much pressure is required to deform the front of the eye => one of the reasons that you tend to get blockages is that the ciliary muscle gets bigger => folds back and occludes the drainage channels => can't get them to contract and thus uncover the drainage channels => to treat, we use a muscarinic receptor agonist like pilocarpine
- Pilocarpine stimulates the ciliary muscle => which will then pull back from the drainage channels and allow the aqueous humour to flow out => physically opening up the drainage channels by opening up drainage angle => role of ciliary muscle is to control lens => when muscle contracts => lens becomes fatter => focused on near vision => when pt is given pilocarpine for glaucoma => eye becomes permanently focused on near objects => distant vision becomes blurred
- Parasympatholytics
Annotations:
- Muscarinic receptor antagonists => also known as parasympatholytics or anti-cholinergics Lot's of drugs available, including some quite old ones => however limited clinical efficacy due to limited selectivity
- Several of these drugs are plant compounds that were used in traditional herbal remedies => these are tertiary ammonium compounds => they tend to act in the periphery => don't cross the BBB
- Muscarinic receptor antagonists are used to: => dilate the pupil (mydriasis) => e.g. if have glass in eye => want to see inside eye => first thing to do is to dilate pupil => two ways to do this => adrenaline is ok => but doesn't have profound effect => need to switch off parasympathetic ns to get really good dilation => however, does have problems => vision becomes blurred => too much light can trigger painful headaches => can increase intraocular pressure - is dangerous in glaucoma => also causes paralysis of ciliary muscle (cycloplegia) => causes dry mouth and skin => can speed up low heart rate (tachycardia) => can dilate airways (bronchodilation) => stops constricting effect of parasympathetic ns => can be used to treat diarrhoea => inhibits gastric motilty and gastric secretion => also used to inhibit bladder emptying (urinary retention) => causes CNS excitation => pt may feel restless, agitated or disorientated
- Atropine
Annotations:
- Comes from the plant Atropa belladonna => commonly known as Belladonna or Deadly Nightshade => the name Belladonna means beautiful lady in italian => Atropine extract eyedrops were used in the middle ages => caused dilation of the pupils => was considered attractive => however, it affected their ability to see => because eye was forced to dilate => near vision became blurry => this could cause severe glaucoma and eventually blindness => not a harmless cosmetic drug
- it's affects lasted about 36 hours => don't use very much clinically any more => don't want pt's vision compromised for so long
- Can also use to treat sinus bradycardia => parasympathetic ns is overactive and pt has very low heart rate => pt will feel rather sluggish and prone to fainting => can use atropine as a muscarinic receptor antagonist to block the ps ns and therefore increase heart rate
- Tropicamide
Annotations:
- Used to dilate pupils (mydriatics) => better than atropine => only lasts for about 40 mins (vs. about 36 hours for atropine)
- Atrovent
Annotations:
- Ipratropium Br => used in asthma and COPD=> there is a subset of pt's where their asthmatic response is due to overstimulation of ps ns on the airways => these pt's will respond to these muscarinic receptor antagonists => note that these drugs are not very selective => can cause side effects => get around this problem by administering them via inhalation => drug tends to stay in airways => so will have effect in lungs but doesn't get in substantive amounts into the blood stream where it would cause side effects
- Dicycloverine
Annotations:
- an antispasmodic drug => used to treat spasms and cramps in the GI tract
- Enter text here
- Parasympathomimetics
- NAChR
- Removal Mechanisms
- Anticholinesterase Drugs
Annotations:
- The enzyme AChE, which removes the ACh from the synaptic cleft, can be inhibitied by a number of drugs (e.g. neostigmine, edrophonium) => these drugs prevent the breakdown of ACh => increase the concentration of the neurotransmitter at the neuromuscular junction
- Can be used to reverse the effects of non-depolarizing muscle relaxants(reversible, competitive antagonists) like tubocurarine and atracurium => overcomes their effect by increasing the concentration of the antagonist Neostigmine in particular is used after surgery to speed up recovery from the muscular blockade that is produced by the non-depolarizing muscle relaxants => Note: does NOT work on depolarizing muscle relaxants (link to them in red)
- In the case of anticholinesterase overdose, it can act as a depolarizing muscle relaxant => paralysis will occur because the neurotransmitter is not rapidly being destroyed so the sodium channels are being kept in a depolarized state by the activation of the receptors and they have no chance to cycle through the refractory period
- Link to non-dep mr
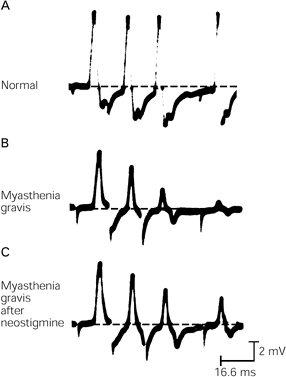
- Use in Myasthenia Gravis
Annotations:
- Myasthenia Gravis is an autoimmune disease characterized by muscle weakness => caused by antibodies destroying the NAChRs at the neuromuscular junction => so the pt's have fewer than normal receptors at the NMJ => so they get very weak muscles because the contractions end up much weaker because of the lack of receptors available to fire off the epp => as can be seen on associated picture, in MG there is an initial response but very quickly dies off because there are not enough receptors to keep the activation going
- Can use neostigmine to combat this => allows ACh to hang around longer => maximized the opportunity for ACh to activate those receptors that are there
- link to dep mr
- Anticholinesterase Drugs
- Receptors
- Pre-junctional
Events in
Cholinergic
Neurotransmission
Annotations:
- Acetylcholine is synthesized from Choline, which has to be taken up from the extracellular space by a transport molecule because the nerve terminal can't manufacture it, and Acetylcoenzyme A (AcCoA) The key enzyme involved in this synthesis is Choline Acetyl Transferase (CAT) => takes a choline molecule and takes an acetate group from the coenzyme AcCoA => joins together to form acetyl choline
- The ACh is then stored in synaptic vesicles that are released by the process of exocytosis => triggered by a rise in the intracellular calcium concentration within the nerve terminal It is very important for the neurotransmitter to be packaged into a vesicle for two reasons: => it is only released in response to an action potential if it is packaged => also, any neurotransmitter that is not packaged into a vesicle gets destroyed => incredibly hostile environment => until it gets packaged into vesicles it can be broken down by esterase enzymes present in the cytoplasm
- Post-junctional
Events in
Cholinergic
Neurotransmission
Annotations:
- The release of ACh into the synaptic cleft is a rapid transmission event => happens very fast => ACh has a very short lifetime in the synaptic cleft => 1-2 ms
- Once released, ACh must make its way across the synaptic cleft to activate the nicotinic ACh receptors (NAChR) => however, in the cleft is the enzyme acteylcholine-esterase (AChE) which breaks the neurotransmitter down => most of the ACh never reaches the NAChR => gets released and is destroyed by AChE before it can get there => AChE is extremely efficient at destroying ACh => most of the ACh molecules that do get to the receptor get destroyed as soon as they come off the receptor => only get one chance to activate the receptor => so an action potential leads to a so-called 'puff' of ACh that is rapidly removed by AChE
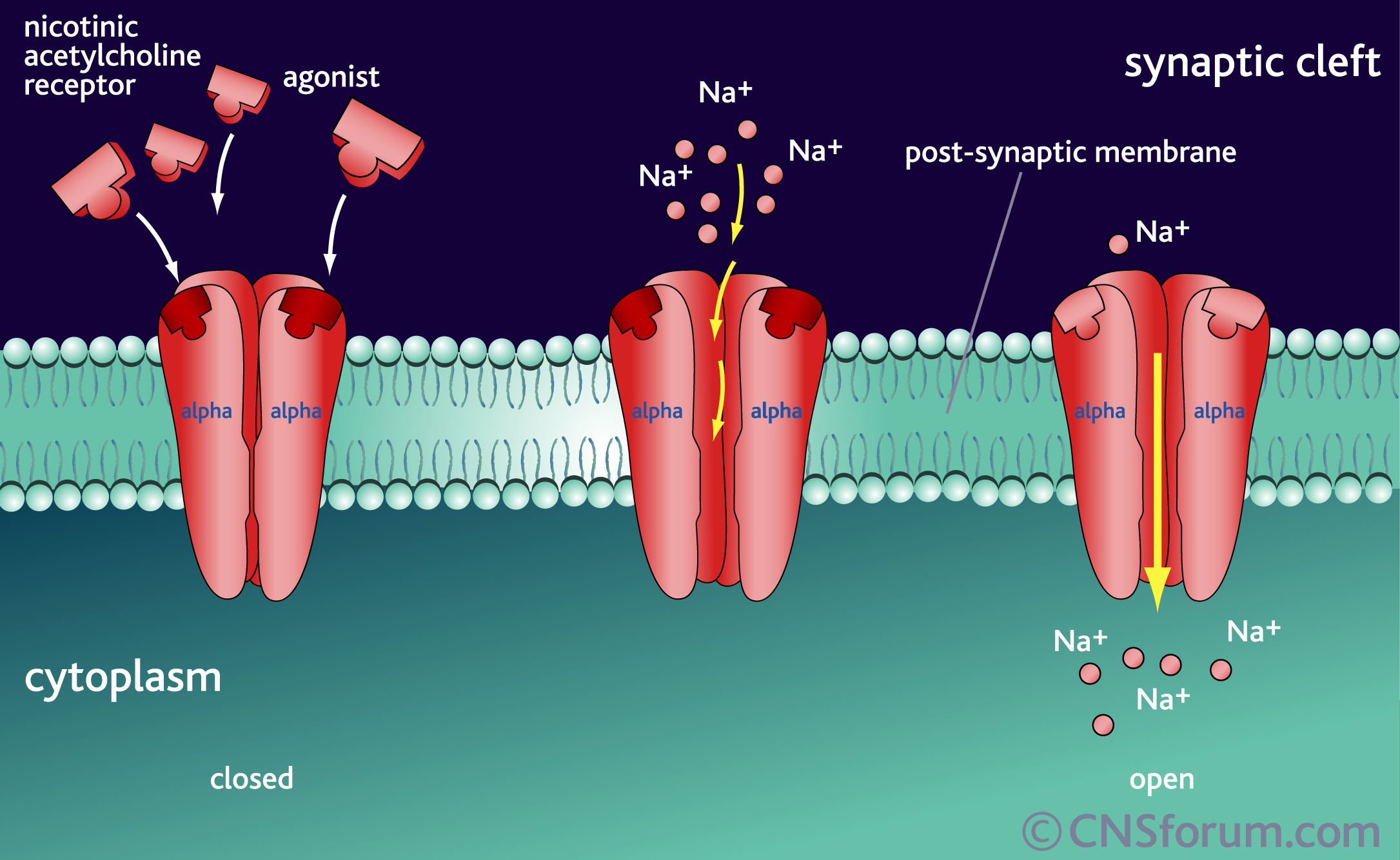
- Nicotinic ACh Receptor
Annotations:
- Referred to as the Nicotinic receptor because nicotine is an agonist => note: nicotine is an exogenous substance => comes from outside the system
- Receptor is formed of five subunits which form around a non-selective cation channel => permeable to Na, K & slightly to Ca => subunits are alpha, alpha, beta, gamma, epsilon (gamma is replaced by another epsilon in foetal muscle) The nicotinic receptors can be broadly distinguished into 3 subtypes: muscle, ganglion and CNS => have slightly different subunits => but always 5 subunits => subunits differ slightly depending on where in the body they are => e.g. in the brain v.s. pns => still 5 subunits but vary slightly This variance leads to a difference in pharmacology between the receptors => add slide 5 here
- The channel opens when two ACh molecules bind to the protein complex, one to each alpha subunit => because of this, there must always be two alpha subunits in the receptors => there can be variance between them but this fact cannot change => otherwise receptor will not function correctly Activation of this receptor triggers off sodium entry into the muscle membrane and the membrane depolarizes
- The depolarisation of the muscle membrane produced following the activation of the NAChR is called an end-plate potential (epp) => the role of the epp is to get the membrane to the threshold at which the muscle membrane fires off an action potential => spreads across the muscle and ultimately causes contraction => it's like the trigger for the AP
- Not all drugs that work on nicotinic receptors work on all subtypes => tubocurarine only affects muscular nicotinic receptors => add this to end of slide 2
- Muscle subtype
Annotations:
- Located at the somatic NMJ Subunits are: (alpha1)2, beta1, delta and epsilon ACh is an agonist as well as nicotine (although it is not great) Tubocurarine and pancuronium are both antagonist => selective for this subtype of receptor => they are both effective muscle relaxants
- Ganglion subtype
Annotations:
- Located in the autonomic ganglia (both in the sympathetic and parasympathetic ns) Subunits are: (alpha3)2 and (beta4)3 Acetylcholine is an agonist as well as nicotine and dimethylphenylpiperazinium (DMPP) Have antagonists such as hexamethonium and trimetaphan (although it has very different clinical action) => however, because these receptors are present in the whole of the autonomic ganglia => they have an extremely widespread effect => so they are not very useful clinically because of the widespread side effects
- CNS subtype
Annotations:
- Located in the brain Subunits are either : (alpha4)2 and (beta2)3 or (alpha7)5 Agonists are ACh, nicotine and DMPP No known antagonists => but is being researched => could be useful for treatment of nicotine dependance
- Muscarinic ACh Receptors
Annotations:
- Located at the NEJ in the parasympathetic ns and at the NEJ of the sweat glands in the sympathetic ns Completely different structure to the nicotinic receptors The name muscarinic comes from the compound muscarine => comes from a toadstool => historically was shown to be able to activate these receptors
- Structurally quite different to NAChR => are G-protein coupled receptors => has 7 transmembrane proteins => has the N-terminus which is outside the cell and the C-terminus inside the cell => when the receptor is activated, the receptor interacts with this G-protein which is down by the C-terminus
- This is not an ion channel, like the nicotinic receptor => activation of receptor leads to cascade of biochemical events, mediated by this G-protein
- There are 5 subtypes of the muscarinic receptor: M1, M2, M3, M4, and M5 => however, pharmacologically can only tell the difference between M1, M2 and M3 => not sufficient difference for drugs to differentiate further => this is likely because the structural difference that differentiates M4 and M5 from the others is probably not in the area where the receptor is
- Quite difficult to get drugs that are absolutely selective for one subtype => despite drug companies spending years on research
- M1 Receptor
Annotations:
- Main role, as far as the periphery is concerned, is regulating the release of gastric acid (hydrochloric acid) from the parietal cells ACh either binds to M1 receptors on the enterochromaffin-like (ECL) cells which in turn activate the parietal cells or ACh can bind directly to M3 receptors on the parietal cells, but this produces a much weaker response
- ACh is an agonist Atropine is an antagonist Historically, there is a drug called pirenzepine => also an antagonist => was used to treat gastric ulcers => it was blocking these M1 receptors => treating the excessive gastric acid secretion
- However, as can see from diagram => when blocking M1 receptor, there are still other ways to induce acid secretion => best way to block it is to block the proton pump => need a proton pump inhibitor => e.g. omeprazole => much more effective => is acting right at the end of the pathway where all the various pathways come together
- There are also some M1 receptors in the brain => get an excitatory effect => excite nerve cells
- When you activate M1 receptors => trigger off a biochemical cascade involiving Inositol triphosphate (IP3) and Diacylglycerol (DAG) => get an increase in intracellular concentration of calcium inside the target cell => that initiate the final response
- insert pictures
of parietal
cells (notes)
- PLC/IP3/DAG Pathway
Annotations:
- M1 and M3 both follow this biochemical pathway => they are on different cells, but the reaction is the same
- So ACh activates the muscarinic receptor (M1/M3) => stuck inside the cell membrane (near the C-terminus of the receptor) is the g-protein, which has 3 subunits (alpha, beta, gamma) => the 7 transmembrane proteins form a sort of pocket, into which ACh falls => so when the receptor becomes activated, the alpha subunit of the g-protein stays by the receptor, while the beta and gamma units float off to do something else => the alpha subunit can then trigger off different responses inside the cell => depending on which g-protein is involved => in this case, the g-protein is called Gq This Gq-protein then activates an enzyme called phospholipase C => that lipase then breaks down a phospholipid in the membrane called PIP2 => takes off the phosphate head group (IP3) and leaves the lipid (DAG) behind => both IP3 and DAG are biologically active substances => DAG activates an enzyme called protein kinase C (PKC) => which goes on to phosphorylate a whole host of target proteins in the cell IP3 goes to the endoplasmic reticulum of the cell => causes the release of calcium ions from the endoplasmic reticulum => this calcium goes on to do a whole host of different things => lots of calcium dependant responses (e.g. smooth muscle contraction, secretion in gastric secretion cells)
- Continual activation of PKC is involved in abnormal cell devision => is a target for cancer research => drugs that inhibit PKC are being developed as anti-cancer drugs
- Pathway diagram
- M2 Receptor
Annotations:
- Really only found of any significance in the heart
- Main thing they do is slow down heart rate => also inhibit nerve cell function in the CNS
- They down-regulate the function of cyclic AMP
- If you stimulate the vagus nerve => which is the parasympathetic nerve that release ACh on the heart => the ACh is going to activate the muscarinic receptors => slows down heart (see diagram) => switch of the vagus nerve and it goes back up again => what happens is that the M2 receptors open potassium channels and hyperpolarize the cell membrane of the pacemaker of the hear, the SA node => so the main role of M2 receptors is slowing down of the heart
- Adenylyl
cyclase -
cAMP pathway
Annotations:
- In this pathway, the g-protein is called Gi (vs. Gq) => the alpha subunit here inhibits the enzyme adenylyl cyclase -Inside cell adenylyl cyclase is constantly being regulated => what it does is take ATP and manufacture cyclic AMP from it=> so cAMP concentration goes up and it activates protein kinase A (PKA) => PKA phosphorylates different target proteins So to control the activity of adenylyl cyclase, we have two routes of action: => we can inhibit it's action by using the Gi-protein => e.g. through M2 muscarinic receptors => we can also stimulate the activity of adenylyl cyclase by using the Gs-protein (s for stimulates) => which is activated by beta adrenoreceptors in the sympathetic nervous system => so can tightly control the activity using those two pathways
- pathway diagram
- diagram - ps effect on heart
- M3 Receptor
Annotations:
- Affects => eyes: pupil constriction, ciliary muscle constriction Lacrimal and salivary glands => secretion Lungs => airway constriction, secretion from glands GI tract => smooth muscle - increase motility, dilation of sphincters, secretion from glands (note gastric acid secretion is controlled by M1) Bladder => smooth muscle contraction, relaxation of sphincters Genetalia => dilation of blood vessels (erection)
- Same second messenger pathway as M1 receptors
- Link to PLC/IP3/DAG
- Sympathetic NS
Annotations:
- Sympathetic nerves leave the spine in the middle (thoracic and lumbar flow) The preganglionic nerves are short while post-ganglionic are long => so because the preganglionic nerves are short, the ganglions are very close to the spine => there is a chain of ganglion on either side of the spinal cord (sympathetic chain)
- Affects eyes, airways, salivary glands, heart, GI tract, bladder and reproductive organs Sympathetic NS also innervates the adrenal medulla => gland that secretes adrenaline and noradrenaline into the blood stream when stressed
- At ganglions and at adrenal medulla (which has no ganglion), sympathetic ns, has exclusively acetylcholine acting on nicotinic receptors At neuroeffector junction however, have a more variability between receptors => most common is that noradrenaline is the neurotransmitter => it acts on alpha (1 & 2) and beta (1 & 2) receptors => there are different types of noradrenergic receptors in different organs
- Both Noradrenaline and Adrenaline act as agonists => are activated from a mixture of neurotransmitters from nerves and circulating adrenaline from the adrenal medulla
- Sweat production is governed by the sympathetic NS => the sympathetic nerves that act on the sweat glands are the only ones that release acetylcholine that acts on muscarinic receptors
- Sympathetic NS is the branch of the nervous system that governs the fight/flight response => increased heart rate & more force => get more oxygenated blood around the body (in particular to skeletal muscle) =>salivary glands => (e.g. before exam) get dry mouth => get thick, viscous secretion => airways dilate => get more O2 => eyes => pupils dilate => GI tract => decreased peristalsis and secretions => don't need to digest when in danger
- link to ganglion stimulants
- Enteric NS
Annotations:
- Covers the function of the GI tract
- Afferent Nerves
Annotations:
- These are most often sensory nerves => carry information to the CNS from the PNS
- Efferent Nerves
Annotations:
- Carry information away from CNS
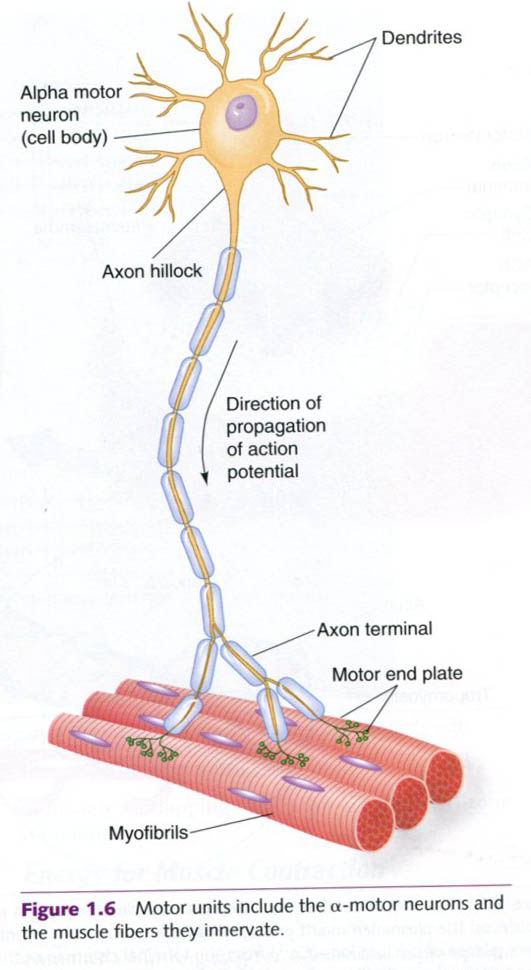
- Motor unit
Annotations:
- When we want to move our arm => action potential moves don motor nerve and innervates the skeletal muscle => the nerve and the muscle it controls is know as the motor unit
- The number of muscle fibres per motor unit differs according to the delicacy of the movement required => for fine movements, e.g. in the finger => want to be able to make very slight incremental changes => each muscle nerve only innervates a few muscle fibres => delicate increases in the amount of tension => compared to muscles in legs => don't need to be very fine => have several hundreds of muscle fibres controlled by a single nerve
- Neuromuscular Junction
Annotations:
- Specialized region where nerve meets muscle => nerve sits in indentation => like a cup where the nerve sits => folds in the muscle end-plate (a specialized region in the muscle membrane, where transmission occurs) increase the surface area
- Terminal Schwann cell forms cap over junction => this is important from a pharmacological point of view =>makes it difficult to get drugs into the synapse => very restricted region 'Gap' between nerve and muscle is about 60 nm => neurotransmitters have to be able to diffuse across this 'gap' to activate receptors on the muscle end-plate
- Neurotransmission
Annotations:
- Initial steps are the same all the time => just differs what neurotransmitter is released and what receptor it activates
- Action
potential in
presynaptic
neurone
Annotations:
- Action potential shoots down nerve
- Depolarization
of nerve
terminal
- Opening of
Voltage-Operated
Calcium Channels
Annotations:
- These are the really important channels => without these the signal wouldn't travel across the synapse => allow release of neurotransmitters => link depolarisation of membrane (i.e. the action potential) to changes in biochemical activity inside the cells
- Calcium entry
into Nerve
Terminal
Annotations:
- Get a rise in intracellular calcium concentration at the nerve terminal region => stimulus for activation of neurotransmitter
- Release of
Neurotransmitter
by exocytosis
- Activation of
Post-Synaptic
Receptors
- Somatic Nervous System
Media attachments
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Want to create your own Mind Maps for free with GoConqr? Learn more.