325369
Description
Mind Map by Daniel Elandix G, updated more than 1 year ago
|
|
Created by Daniel Elandix G
about 11 years ago
|
|
H. Pylori and Peptic Ulcer Disease
- Anatomy
- Stomach
Annotations:
- Can be divided into 4 parts Cardia, fundus, body and anthrum (pylorus) Function: 1. Temporary food storage 2. Control the rate of which food enters the duodenum 3. Acid secretion 4. Fluidsation of stomach content 5. Preliminary digestion with pepsin lipase's etc.
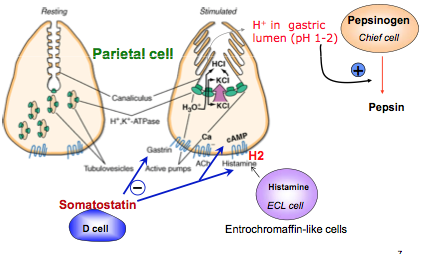
- Parietal Cells
Annotations:
- Control of gastric acid secretion is done by various stimuli and control via neural, endocrine and paracrine. I.e Muscarinic via ACh Gastrin receptors via gastrin Histamine (stimulant to release ACh and gastrin)
- Stomach
- Peptic Ulcer Disease
Annotations:
- A collection of disease that cause a disruption of the mucosal integrity of the stomach, duodenum, or both and it's being caused by local inflammation.
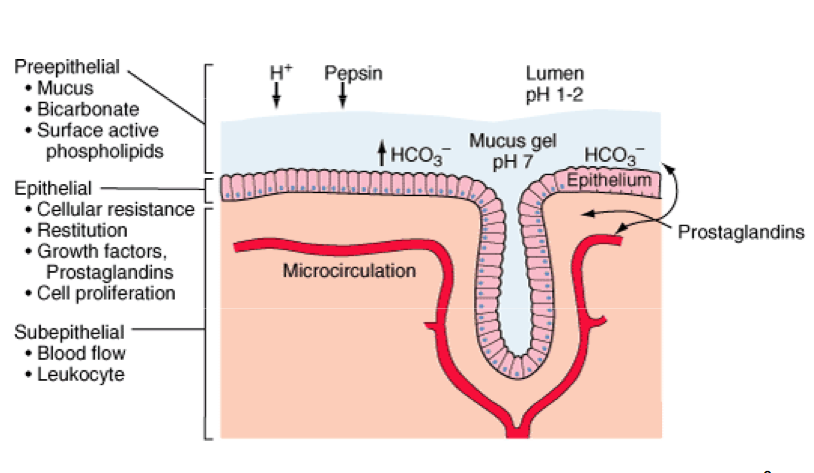
- Gastroduodenal Mucosal Defense
Annotations:
- Various layers of protection. Basically a physical and physiological barrier. From mucus to leukocytes
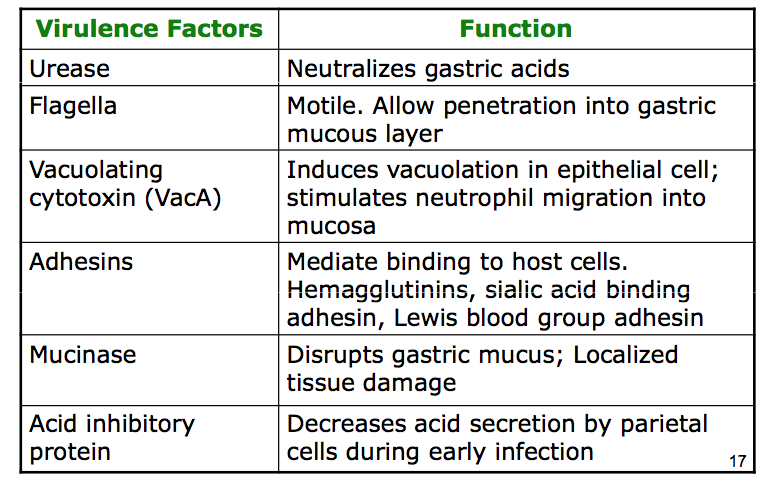
- Helicobacter Pylori
Annotations:
- Bacterium that is the major cause of peptic ulcers. Gram negative, motile and able to survive in acidic environment. Found in 50% of people worldwide.
- Physiological Factors
Annotations:
- Helicobacter lives in the lining of the mucus (mucus protects the lining of stomach against the acid) It also contains urease that buffers local pH.
- Effect on the Stomach
Annotations:
- It enters the mucus layer and adhere to the gastric epithelial cells. It weakens the protective mucus coating of the stomach and duodenum and triggers inflammatory response (gastritis). Less mucus and lowered protection of the host cells to acid. Then it cause an ulcer, if continued inflammation, adenocarcinoma will occur. MALT (Mucosa-associated lymphoid tissue) can progress to gastric lymphoma.
- Symptoms
Annotations:
- Many patients are asymptomatic. Pain is the most common symptom (mild-moderate pain) Desciption of pain is, burning, gnawing or hunger, can be relieved by eating or antacids. Ulcers may bleed, leading to haematemesis.
- Diagnostics
Annotations:
- 1. Urease breath test: Simple and quick. The patients ingest water containing C-urea and the breath is then examined for 14Co2. 2. Blood Tests: Detection of antibodies to H.pylori 3. X-ray: Barium meal, then it outline lining of the stomach wall. Makes ulcer visible. 4. Endoscopy: Camera to either the ass or mouth. 5. Stool test: Check for antigen (used for children)
- Causes
Annotations:
- May be NSAID Smoking Excessive alcohol consumption Stress
- Drugs
Annotations:
- Best is to inhibit proton pump Or to block cholinergic transmission (last resort)
- Antacids
Annotations:
- Mylanta or rolaids Weak bases Aluminium hydroxide and magnesium hydroxides Relieve symptoms by neutralising stomach acid.
- Anti-acid Secretion Agents
Annotations:
- Competitive and selevive inhibition of histamine H2 receptors. They suppress 25hr gastric secretion by 70%
- PPI
Annotations:
- Proton Pump inhibitor
- Eradication Treatment
Annotations:
- Combination of antibiotics and PPI. Some causes for effectiveness are low compliance or bacterium resistance to antibiotics.
Media attachments
{kind=link}
{kind=link}
{kind=link}
Want to create your own Mind Maps for free with GoConqr? Learn more.