6645257
Description
Flashcards by Andrew Street, updated more than 1 year ago
|
|
Created by Andrew Street
about 8 years ago
|
|
| Question | Answer |
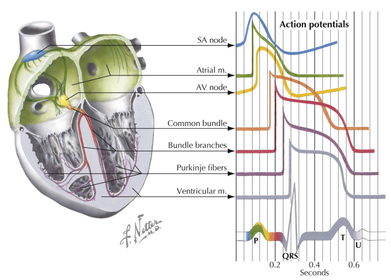
| 1062 Outline the conduction system of the HT & how this relates to the waves seen on an ECG. | |
| 1021 Describe the presentation of someone with arrhythmias. | Presentation: * Palpitation * CP * Presyncope/syncope * Hypotension * Pulmonary oedema * Some arrhythmias may be asymptomatic & incidental, eg AF. OHCM p118. |
| DDx for syncope. | * Cardiovascular > MI > PE > Cardiac outflow obstruction > carotid sinus syndrome > Vasovagal syncope - situational, micturation, cough > Orthostatic hypotension - prolonged bedrest, drug-induced, hypovolaemic, autonomic failure > Arrhythmia - SVT, VT, sick sinus syndrome, Stokes-Adams attack * Neurological > Seizure > Hysterical syncope * Metabolic > Hypoxia > Hypoglycaemia DDx p443. |
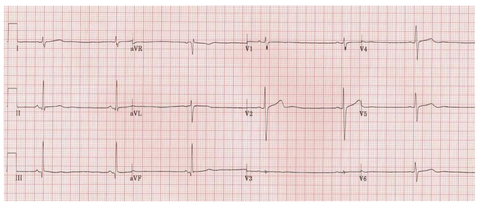
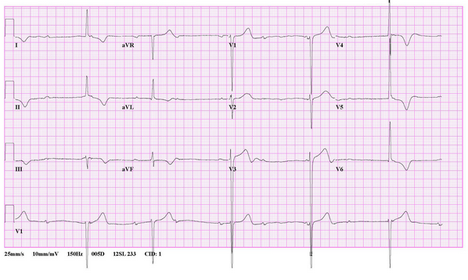
| Sinus bradycardia (35 bpm) in a 15-year old girl with anorexia nervosa. Note the prominent U waves in the precordial leads, a common finding in sinus bradycardia. http://lifeinthefastlane.com/ecg-library/sinus-bradycardia/ | |
| 1025 Give extrinsic & intrinsic causes of sinus bradycardia. | Sinus bradycardia is due to extrinsic factors influencing a relatively normal sinus node or due to intrinsic sinus node DS. The mechanism can be acute & reversible or chronic & degenerative. Common causes of sinus bradycardia include: * Extrinsic causes > Hypothermia, hypothyroidism, cholestatic jaundice, & ^ICP > Drug Rx with beta-blockers, digitalis & other antiarrhythmic drugs > Neurally mediated syndromes - carotid sinus syndrome (elderly, bradycardia -> syncope), neurocardiogenic (vasovagal) syncope (young adults or elderly. Results from effects on autonomic NS, eg emotions, -> bradycardia &/or vasodilaltion), postural orthostatic tachycardia syndrome (peripheral vasculature fails to respond appropriately to changes in BP -> sudden & significant ^HR). * Intrinsic causes: > Acute ischaemia & infarction of the sinus node (as a complication of acute MI) > Chronic degenerative changes such as fibrosis of the atrium & sinus node (sick sinus syndrome). K & C p698. |
| Rx of sinus bradycardia. | * Identify & remove any extrinsic cause * Temporary pacing - for pt's with reversible causes or pt's with chronic causes awaiting permenant pacing * Permenant pacing - pt's with chronic sick sinus syndrome, carotid sinus hypersensitivity, malignant neurocardiogenic syncope. k & C p699. |
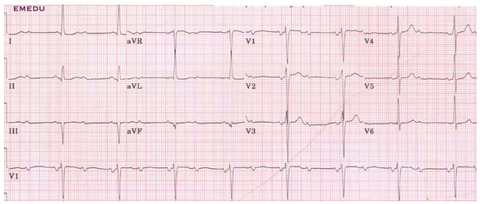
| First degree HT block. PR interval >200ms. | |
| In complete HT block (third degree), there is complete absence of AV conduction – none of the supraventricular impulses are conducted to the ventricles. Perfusing rhythm is maintained by a junctional or ventricular escape rhythm. Alternatively, the pt may suffer ventricular standstill leading to syncope (if self-terminating) or sudden cardiac death (if prolonged). Typically the pt will have severe bradycardia with independent atrial & ventricular rates, i.e. AV dissociation. http://lifeinthefastlane.com/ecg-library/basics/complete-heart-block/ | |
| AV Block: second degree type I, Mobitz I (Wenckebach Phenomenon) Progressive PR interval culminating in a non-conducted P wave The PR interval is longest immediately before the dropped beat The PR interval is shortest immediately after the dropped beat. http://lifeinthefastlane.com/ecg-library/basics/wenckebach/ | |
| Complete HT block. | |
| Second degree type II (Mobitz II) – The finding is again best visible in the long recorded lead (this time V1 lead). We see two P waves between every two QRS complexes. One P wave normally precedes the QRS complex and the second is alone – its QRS complex is missing. http://www.health-tutor.com/second-degree-av-block-ecg.html | |
| Rx for first & second degree HT block. | * First degree - usualy not treated unless symptomatic * Second degree type I (wenkebach phenomenon) - as block is in AV node Mx is usually just monitoring * Second degree type II - block is infra-nodal in His bundle with risk of progression to third degree block so pacing recommended. K & C p699. |
| Rx of third degree (complete) HT block. | Generally permanent pacing or ICD especially if symptomatic, chronic, associated with HT DS, severe bradycardia, or broad complex escape rhythm. K & C p700. |
| RBBB - delayed RV activation produces a secondary R wave (R’) in the R precordial leads (V1-3) & a wide, slurred S wave in the lateral leads. http://lifeinthefastlane.com/search/?q=right+bundle+branch | |
| Incomplete RBBB is defined as an RSR’ pattern in V1-3 with QRS duration < 120ms. It is a normal variant, commonly seen in children (of no clinical significance). In this eg - incomplete RBBB (RSR’ pattern in V1) in a 2-year old child. http://lifeinthefastlane.com/ecg-library/basics/right-bundle-branch-block/ | |
| Causes of RBBB. | * RVH / cor pulmonale * PE * IHD * Rheumatic HT DS * Myocarditis or cardiomyopathy * Degenerative DS of the conduction system Congenital HT DS (e.g. atrial septal defect). http://lifeinthefastlane.com/ecg-library/basics/right-bundle-branch-block/ |
| * In LBBB, the normal direction of septal depolarisation is reversed (becomes R to L), as the impulse spreads first to the RV via the R bundle branch & then to the LV via the septum. * This sequence of activation extends the QRS duration to > 120 ms and eliminates the normal septal Q waves in the lateral leads. * The overall direction of depolarisation (from R to L) produces tall R waves in the lateral leads (I, V5-6) & deep S waves in the R precordial leads (V1-3), & usually leads to L axis deviation. * As the ventricles are activated sequentially (R, then L) rather than simultaneously, this produces a broad or notched (‘M’-shaped) R wave in the lateral leads. http://lifeinthefastlane.com/ecg-library/basics/left-bundle-branch-block/ | |
| Causes of LBBB. | * Aortic stenosis * IHD * HT * Dilated cardiomyopathy * Anterior MI * Primary degenerative disease (fibrosis) of the conducting system (Lenegre disease) * Hyperkalaemia * Digoxin toxicity. http://lifeinthefastlane.com/ecg-library/basics/left-bundle-branch-block/ |
| S, Sx & Rx of bundle branch blocks. | * Usually asymptomatic * Syncope may be experienced in pt's with intraventricular conduction disturbances Rx any underlying causes. New onset LBBB with Sx of CP is Rx as ACS. K & C p701 & OHCM p112. |
| SVT's arise from the ..... or the ..... junction. Conduction is via the .....-..... system; therefore the QRS shape during tachycardia is usually ..... to that seen during baseline rhythm. | SVT's arise from the atrium or the atrioventricular junction. Conduction is via the His–Purkinje system; therefore the QRS shape during tachycardia is usually similar to that seen during baseline rhythm. K & C p702. |
| S & Sx of SVT's. | * Palpitations - no. 1 Sx (esp AVNRT & AVRT). Palpitations may be: > Regular - AVNRT & AVRT > Irregular - atrial premature beats, atrial flutter, AF, or multifocal atrial tachycardia * Hypotension * Dizziness * Syncope * Anxiety * Dyspnoea * CP * Weakness * S & Sx of CHF - esp AF with reduced ventricular function * Neck pulsations. K & C p704. |
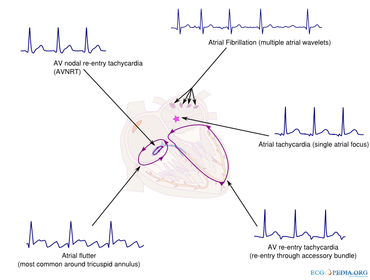
| List causes of SVT's. | * Sinus tachycardia * AV nodal re-entry tachycardia (AVNRT) - commenest cause of palpitations in pt's with healthy HT's * AV re-entry tachycardia (AVRT) * AF - commonest tachycardia in >65 YO's * Atrial flutter * Atrial tachycardia - usually associated with structural HT DS * Multifocal atrial tachycardia - rare, associated with significant lung DS. K & C p702. |
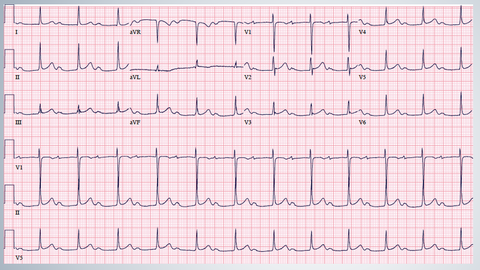
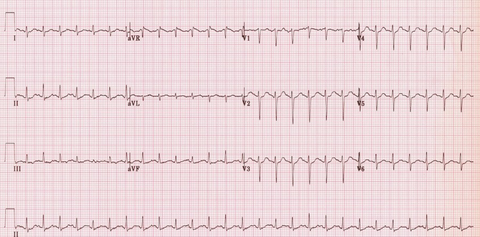
| Sinus tachycardia: HR 150 bpm. P waves are hidden within each preceding T wave. http://lifeinthefastlane.com/ecg-library/sinus-tachycardia/ | |
| List causes & Rx of sinus tachycardia. | Acute: * Exercise * Emotion * Pain * Fever * Infxn * Acute HF * Acute PE * Hypovolaemia Chronic: * Pregnancy * Anaemia * Hyperthyroidism * Catecholamine excess Rx - find & Rx the underlying cause. If neccessary use beta-blockers to slow sinus rate eg in hyperthyroidism. K & C p702. |
| Explain the conduction pathways in the HT in AVNRT & AVRT. | |
| AVNRT P wave is often not visible as buried in the QRS. ECG At A Glance p105. | |
| AVRT This is an orthodromic AVRT (the more common variant). The current passes through the AV node, into the ventricles, then returns back up the accessory pathway causing a lat retrograde P wave. ECG At A Glance p107. | |
| WPW An accessary pathway causes a reduced P-R interval & pre-excitation of the ventricles (delta wave). R axis deviation and a dominant R wave in V1 may be seen. There may be a sinus rhythm or if a re-entry circuit forms it can cause a paroxysml tachycardia. ECG At A Glance p107 & ECG Made Easy p80. | |
| Mx of SVT's. | * In an emergency distinguishing between AVNRT & AVRT isn't important as the Rx is the same * If haemodynamically unstable - 'IV adenosine. Initial 6mg dose over 2 secs. If no effect within 1 min give second injection of 12mg. Further doses are not recommended. If the pt is refractory to drugs seek advice. All supraventricular arrhythmias may be Rx by ablation. Patients who have syncope due to WPW syndrome or atrial flutter with 1:1 conduction, should be referred immediately to the cardiology registrar on call and considered for urgent in-pt ablation. Any other pt who has an episode of atrial flutter or junctional re-entry tachycardia should be referred to an interventional electrophysiologist as an outpt so that Rx by ablation can be discussed. Pt's with recurrent & highly symptomatic AF should also be referred.' Greybook. * If haemodynamically stable - valsalva manoeuves. k & C p704. |
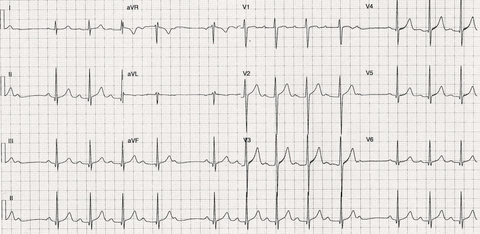
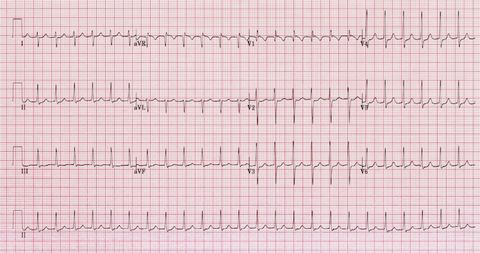
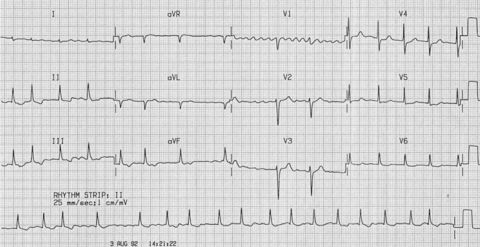
| Key features of AF: * Irregularly irregular rhythm. * No P waves. * Absence of an isoelectric baseline. * Variable ventricular rate. * QRS complexes usually < 120 ms unless pre-existing bundle branch block, accessory pathway, or rate related aberrant conduction. * Fibrillatory waves may be present & can be either fine (amplitude < 0.5mm) or coarse (amplitude >0.5mm). Fibrillatory waves may mimic P waves leading to misdiagnosis. In this ECG we see: * Irregular ventricular response . * Coarse fibrillatory waves are visible in V1. * “Sagging” ST segment depression is visible in V6, II, III & aVF, suggestive of digoxin effect. http://lifeinthefastlane.com/ecg-library/atrial-fibrillation/ | |
| Atrial fibrillation: Irregular ventricular response. Coarse fibrillatory waves are visible in V1. http://lifeinthefastlane.com/ecg-library/atrial-fibrillation/ | |
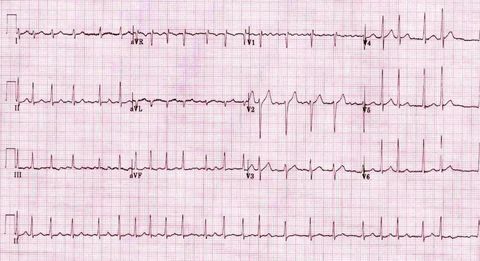
| AF with rapid ventricular response Irregular narrow-complex tachycardia at ~135 bpm. Coarse fibrillatory waves in V1. http://lifeinthefastlane.com/ecg-library/atrial-fibrillation/ | |
| S & Sx of AF. | * Sx highly variable - in 30% it's an incidental finding ie asymptomatic In others there may be: * Rapid palpitations * Dyspnoea * CP. K & C p705. |
| Name the causes of AF. | * HF * Hypertension * MI (seen in 22%) * PE * Mitral valve DS * Pneumonia * Hyperthyroidism * Caffeine * Alcohol * Post-op * Hypokalaemia * Hypomagnesaemia Rare causes: * Cardiomyopathy * Constrictive pericarditis * Sick sinus syndrome * Lung CA * Atrial myxoma * Endocarditis * Haemochromatosis * Sarcoid OHCM p124. |
| Clinical classification of AF. | * First detected * Paroxysmal - stops spontaneously within 7/7 * Persistent - requires cardioversion * Permanent - unresponsive to cardioversion. K & C p705. |
| Mx of acute AF (<48hrs). | If big ill/unstable: * O2 * U & E * Cardioversion - if unavailable try IV amiodarone * Rx associated illnesses * Control ventricular rate - 1st line verapamil (40-120mg/8hrs PO) or bisoprolol (2.5-5.0mg/d PO). 2nd line digoxin or amiodarone. * Start LMWH * If 48 hr period has elapsed cardioversion is ok if confirmed thrombus-free by TOE. OHCM p124. |
| What are the main goals in Mx chronic AF and outline how this is achieved. | Main goals = rate control & anticoagulation. Rhythm control is also appropriate if: symptomatic or CCF, younger, 1st presentation with 'lone' AF (no identifiable cause), or if precipitent has been corrected with no effect (eg hypokalaemia). * Rate control - 1st line beta-blocker or rate-limiting calcium channel blocker. If this fails add digoxin then consider amiodarone * Cardioversion - echo 1st; pre-Rx for ≥4wks with sotalol or amiodarone if there is ↑risk of cardioversion failure (past failure, or past recurrence). Pharmacological cardioversion: flecainide is 1st choice if no structural HT DS (IV amiodarone if structural HT DS). * AV node ablation, maze procedure, pacing, & pulmonary vein ablation are other options * Anticoagulation -see next card. OHCM p124. |
| Outline Mx of anticoagulation in acute AF. | * Heparin until a full risk assessment for emboli is made—eg AF started <48h ago & elective cardioversion is being planned (if >48h, ensure ≥3wks of therapeutic anticoagulation before elective cardioversion). * Warfarin (target INR: 2.5; range 2–3) if risk of emboli ^ (past ischaemic stroke, TIA or emboli; ≳75yrs with BP↑, DM; coronary or peripheral arterial DS; evidence of valve disease or ↓LV function/CCF—only do echo if unsure). * No anticoagulation if stable sinus rhythm has been restored & no risk factors for emboli, & AF recurrence unlikely (ie no failed cardioversions, no structural HT DS, no previous recurrences, no sustained AF for >1yr). OHCM p125. |
| Outline Mx of anticoagulation in chronic AF. | * Warfarin - aim for INR of 2–3 * Aspirin (less good) ∼300mg/d PO - eg if warfarin CI or at very low risk of emboli (<65yrs, and no HT, DM, LV dysfunction, ↑LA size, rheumatic valve DS, MI, or past TIA). |
| What are CI's to warfarin in AF? | ^Bleeding risk diathesis * ^BP - >160/90 (consistently) * Compliance issues - around dosing or INR monitoring * PT choice after risks discussed Factors such as age ≳75–80yrs old, frequent falls, on NSAID's, past intracranial bleeds, Hb↓, & polypharmacy may be considered CI's but are less evidence-based. Discuss with pt: let him decide. The CHA2DS2-VASc score quantifies risk of stroke & may help in decision making. OHCM p125. |
| What factors does the CHADS2VASc score evaluate? | * Congestive HT failure * HT * Age >75 YO * DM * Previous stroke or TIA * Vascular DS - aorta, coronary, or peripheral arteries * Age 65-74 YO * Female Each factor = 1 point, except age > 75 YO & previous stroke or TIA which = 2 points. Score of 2 or more = anticoagulate. ! = consider for anticoagulation or aspirin. K & C p706. |
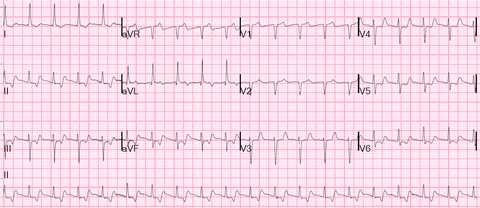
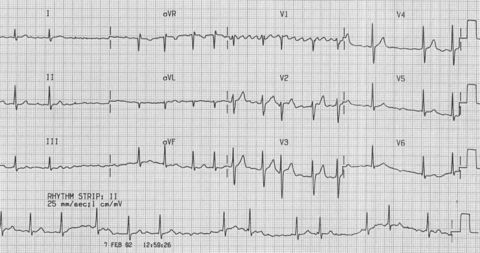
| General ECG features of atrial flutter: * Narrow complex tachycardia * Regular atrial activity at ~300 bpm * Flutter waves (“saw-tooth” pattern) best seen in leads II, III, aVF * Flutter waves in V1 may resemble P waves * Loss of the isoelectric baseline Fixed AV blocks Ventricular rate is a fraction of the atrial rate, e.g. 2:1 block = 150 bpm 3:1 block = 100 bpm 4:1 block = 75 bpm locks can also be variable. In this ECG: * Inverted flutter waves in II, III + aVF at a rate of 300 bpm * There are upright flutter waves in V1 simulating P waves * There is a 2:1 AV block resulting in a ventricular rate of 150 bpm * Note the occasional irregularity, with a 3:1 cycle seen in V1-3. http://lifeinthefastlane.com/ecg-library/atrial-flutter/ | |
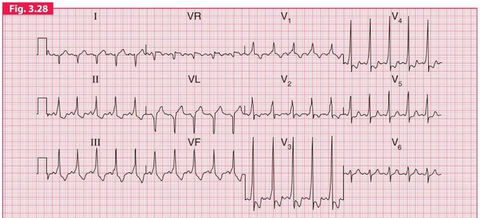
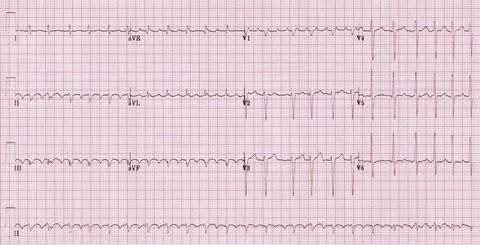
| Atrial Flutter with Variable Block * Inverted flutter waves in II, III + aVF with atrial rate ~ 300 bpm * Positive flutter waves in V1 resembling P waves * The degree of AV block varies from 2:1 to 4:1 http://lifeinthefastlane.com/ecg-library/atrial-flutter/ | |
| Mx of atrial flutter. | * Rx of a symptomatic acute paroxysm - cardioversion. If more than 1-2 days Rx as AF (anticoagulate for 3/52 prior to cardioversion). * Recurrent paroxysms can be prevented with antiarrhythmics - amiodarone or sotalol * If arrythmia persists - AV nodal blocking agents eg amiodarone * Ablation - for recurrent atrial flutter this is Rx of choice. K & C p707. |
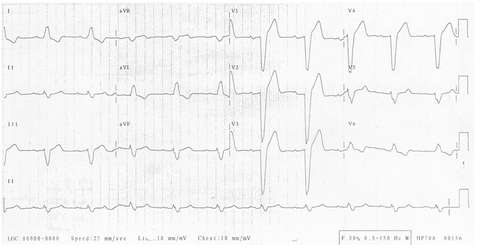
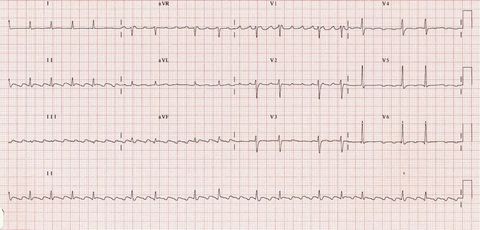
| Ventricular Tachycardia (VT) is a broad complex tachycardia originating in the ventricles. There are several different varieties of VT — the most being Monomorphic VT. In this eg - monomorphic VT: * Classic monomorphic VT with uniform QRS complexes. * Indeterminate axis. * Very broad QRS (~200 ms). http://lifeinthefastlane.com/ecg-library/ventricular-tachycardia/ | |
| Why is VT clinically significant? | * VT may impair cardiac output with consequent hypotension, collapse, & acute cardiac failure. This is due to extreme HR & lack of coordinated atrial contraction (loss of “atrial kick”). * The presence of pre-existing poor ventricular function is strongly associated with cardiovascular compromise. * Decreased CO may result in decreased myocardial perfusion with degeneration to VF. * Prompt recognition and initiation of treatment (e.g. electrical cardioversion) is required in all cases of VT. http://lifeinthefastlane.com/ecg-library/ventricular-tachycardia/ |
| Mx of VT. | If unstable (hypotensive or pulmonary oedema): * Immediate DC cardioversion If stable: * Give high-flow O2 * IV access. Send u&e, cardiac enzymes, Ca2+, Mg2+. Correct low K+or Mg2+. * Obtain 12-lead ecg. * ABG (if evidence of pulmonary oedema, reduced conscious level, sepsis). * Amiodarone IVI. * Rarely, lidocaine 50mg over 2min instead, followed by infusion. * If polymorphic (torsade de pointes) magnesium sulphate 2g over 5min. * If this fails, or if cardiac arrest, use DC shock. * After correction of VT, establish cause from Hx/Ix. * Maintenance antiarrhythmic therapy may be required, eg amiodarone. * Prevention of recurrent VT: implantation of ICD may help. In refractory cases radiofrequency ventricular tachycardia ablation may be tried. OHCM |
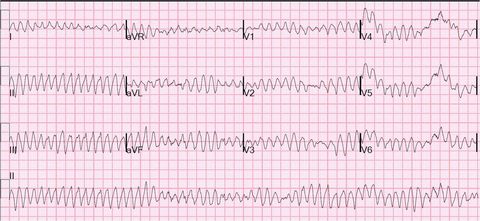
| VF: * Chaotic irregular deflections of varying amplitude * No identifiable P waves, QRS complexes, or T waves * Rate 150 to 500 per minute * Amplitude decreases with duration (coarse VF -> fine VF). http://lifeinthefastlane.com/ecg-library/ventricular-fibrillation/ | |
| Mx of VF. | * Defibrillation * Life support * If survived and no reversible cause (ie MI) then ICD. K & C p708. |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Want to create your own Flashcards for free with GoConqr? Learn more.